|
|
Case Reports Indian Pediatrics 2007;44:856-858 |
||
|
Intracranial Calcification in b-thalassemia Major |
||
|
S. Verma
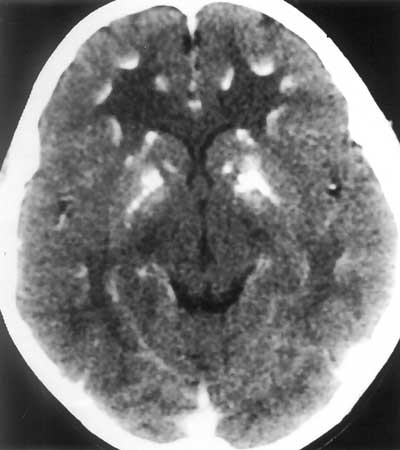
Hypoparathyroidism, Intracranial calcification, Seizure, Thalassemia. Unchelated transfusion dependent b-thalassemia major children are at risk to develop endocrino-pathies(1). Hypoparathyroidism, leading on to hypocalcemia, seizures and tetany is one such well-recognized endocrine disturbance(2). However, metastatic calcification in the central nervous system as a consequence of hypoparathyroidism is an infrequent occurrence in these individuals(3,4). The rarity of the condition prompted us to report this case. Case Report AK, a 13-year-old boy with transfusion dependent thalassemia major presented with generalized seizures. The diagnosis of thalassemia was established in early infancx. He received red cell transfusion at intervals of 2-3 weeks to maintain a pre-transfusion hemoglobin level of 8-9 g/dL, Financial constraints denied him access to iron chelation therapy. Seizure episode was managed with anti-consultants by the local pediatrician. A review of history at our center revealed a developmentally normal child with no past history of seizures. On examination he had pallor, hemolytic facies (prominent frontal, parietal, malar eminences and depressed nasal bridge), greenish brown complexion secondary to pigmentary skin changes and stunted growth with height and weight <5th centile. Spleen and liver were palpable 6 and 4 cm below the right costal margin, respectively. The cardio-vascular examination was normal and there was no neurological deficit. Chovstek and Trousseau’s signs could not be elicited. Investigations confirmed hemoglobin of 8 g/dL, hypocalcemia 7 mg/dL hyperphosphatemia 7.6 mg/dL and alkaline phosphate of 19 KAU. Parathyroid hormone level was 30.30 pg/mL (normal 7-53 pg/mL); it was lower than expected for the degree of hypocalcemia. Computed tomography scan (CT scan) of the head showed multifocal calcification in the gray white junction of both cerebral hemispheres and basal ganglia (Fig. 1). In addition, calcification was seen in bilateral cerebellum including dentate nuclei. EEG had no epileptiform discharges.
Child was put on oral calcium carbonate (1500 mg elemental calcium) and 1, 25 dihydroxycholecal-ciferol (0.25 mg). On subsequent follow-up of 10 months there has been no seizure recurrence. Discussion Hypoparathyroidism in thalassemia major patients has been proposed to be a consequence of iron deposition in parathyroid gland or due to suppression of parathyroid hormone secretion induced by resorption secondary to chronic anemia. Hypocalcemia leading on to tetany, hyperreflexia and seizures is the most common manifestation of hypoparathyroidism. Other biochemical abnormalities include raised phosphate level, near normal alkaline phosphate and normal or low parathyroid levels(1,2). The propositus had all these abnormalities. He had not received any iron chelation therapy whilst receiving over 200 red cell transfusions that resulted in iron overload state. Basal ganglia calcification in hypoparathyroidism has been well documented; however, anecdotal experience of intracranial calcification in individuals with thalassemia is available(3). Karimi, et al. reported 40% (8 out of 20) of their thalassemia patients with hypoparathyroidism had intracranial calcification. All cases were in their second decade of life and had no association between the severity of hypoparathyroidism and extent of intracranial calcification(4). The proposed pathogenesis for metastatic calcification in hypoparathyroidism is from decreased reservoir function of the bone for the absorbed calcium and phosphate from the intestine leading on to extra osseous ca)cification(5). In the basal ganglia this possibly results from a degenerative vascular process in extra-pyramidal system initiated by the deposition of calcium crystals(6). The problems related to calcium metabolism are uncommon in well-chelated transfusion dependent thalassemia patients; however, it would be desirable that unchelated children older than 12 years should have their serum calcium and phosphate levels estimated at regular intervals of 3-6 months. Supplemental therapy with oral calcium and active form of vitamin D would preclude the occurrence of hypocalcaemia related complications. Although routine neuroimaging (CT scan) cannot be recommended, it should be done in children with neurological dysfunction. Contributors: SV and RKM managed the patient; AKS reported the CT scan, SV reviewed the literature and RKM supervised the same. Funding: None. Competing interests: None.
| ||
|
References | ||
|
|
![]()