|
|
Original Article Indian Pediatrics 2005; 42:1092-1100 |
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
Effect of Oil Massage on Growth and Neurobehavior in Very Low Birth Weight Preterm Neonates |
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
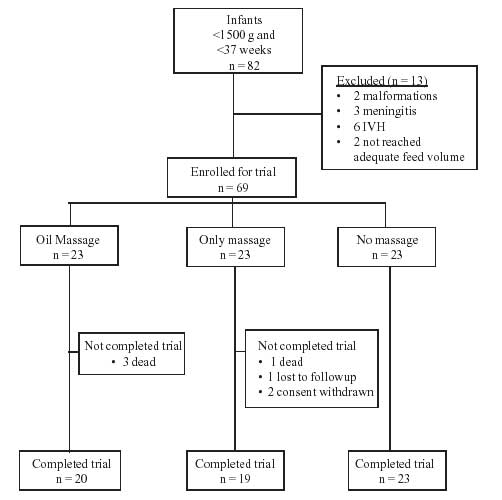
Objective: To study the effect of oil massage on growth and neurobehavior in preterm babies less than 1500 g. Design: Randomized Controlled Trial. Setting: Tertiary level neonatal unit of a teaching hospital. Subjects: Neonates with birth weight <1500 grams, gestation < 37 weeks, receiving enteral feeds of at least 100 mL/kg/day and less than 10 days of age. Outcome variables: Primary-Weight gain 28 days after enrolment. Secondary-Neonatal neurobehavior, change in other anthropometry and serum triglycerides. Methods: Eligible neonates were randomized to one of the three groups (a) massage with oil (b) massage without oil and (c) no massage. Weight, length, head circumference and triceps skin fold thickness were measured in the three groups at regular intervals. Serum triglyceride levels were measured at enrolment and at completion. Neurobehavior using Brazelton’s Neonatal Behavior Assessment Scale (NBAS) was assessed at enrolment and after 10 days of intervention. Results: Weight gain in the oil massage group (365.8 + 165.2g) was higher compared to the only massage group (290.0 + 150.2g) and no massage group (285.0 + 170.4g). This difference and the difference in other anthropometric parameters was not statistically significant. Serum triglycerides and neonatal neurobehavior were comparable in the three groups. Conclusion: Oil application may have a potential to improve weight gain among preterm very low birth weight neonates Key words: Growth, Oil massage, Preterm, Very low birth weight. Massage of infants is widely prevalent in India since times immemorial. Trials on effect of massage on growth in preterm infants have used either massage alone as a form of tactile stimulation or massage with some type of vegetable oil. Oil may act as a source of warmth and nutrition. It is not clear whether oil has any advantage over massage alone on the growth of preterm infants. The present study was designed to test the hypothesis that preterm neonates weighing <1500 g show better weight gain after 4 weeks of massage with oil compared to massage alone. Effect of massage on other anthropometric parameters and neuro-behavior was also studied. Subjects and Methods A randomized controlled trial was conducted in the tertiary level neonatal unit of a teaching hospital. All live intramural births were eligible for inclusion in the trial if they had birth weight <1500 g, gestation <37 weeks and as soon as they received enteral feeds of at least 100 mL/kg/day provided they were less than ten days of age. Neonates were excluded if they had gross congenital anomalies, required supplemental oxygen, inotrope or ventilator support or had intracranial hemorrhage, meningitis or encephalopathy at enrolment. Primary outcome variable: Weight gain 28 days after enrolment into the study. Secondary outcome variables: (a) Neonatal neurobehavior 10 days after enrolment as assessed by Brazelton’s Neonatal Behavior Assessment Score (NBAS)(1), (b) gain in length, head circumference and triceps skin fold thickness 28 days after enrolment and (c) serum triglyceride levels 28 days after enrolment. Sample Size estimation To detect a difference in weight gain of 3 g/kg/day (with a pooled SD of 5 g/kg/day) at an a-error of 5% and b-error of 10%, it was estimated that twenty subjects would be required in each trial arm. Randomization Eligible neonates were randomized to one of the three groups using computer generated random number sequences placed in opaque sealed envelopes. These three groups were (a) massage with oil, (b) massage without oil and (c) no massage. Consent was obtained from the parents at the time of enrolment. Intervention Massage with or without oil: A standardized massage technique (as detailed below) was used for the study. Prior to the onset of study, the technique was standardized by one of the investigators (JA) in a sample population of stable low birth weight neonates. During the study, the massage was done by the investigator as far as possible. Each mother was also trained in use of the technique by the investigator. The initial massages performed by the mothers were supervised till they had acquired the massage skills. During hospital stay, mothers’ compliance was checked regularly by the investigator. Technique of massage(2) The massage was carried out first over both shoulders starting from the neck with the baby in prone position. Then it was carried out from the upper back to the waist. Subsequently, each of the two upper and lower limbs was separately massaged in the supine position. In each area the massage comprised of 20 gentle strokes. The duration of each massage was ten minutes performed four times a day. Infants in the oil massage group received massage with 10 mL/kg/day of sunflower oil (wherein 1 mL oil contains 500 mg of linoleic acid) divided equally between each of the four applications. If babies were discharged from the hospital before completing the trial, mothers were given measured amounts of oil so as to last till their next visit. Infants in the massage alone group were massaged using the same technique but without oil. Infants in the no massage group were handled, fondled and fed by the mothers in the same way as the other two groups but were not allowed to be massaged. Every attempt was made to prevent contamination among the groups by segregating the three groups in separate rooms as far as possible. Axillary temperature was recorded both before and after the massage to check for occurrence of hypothermia during the intervention. All neonates stayed in the hospital for at least ten days after enrolment. In those who were discharged before the completion of the study, the mothers continued the intervention at home and they were followed up twice a week until the end of the trial. At discharge, mothers were explained the usual symptoms of hypothermia including the touch technique of detecting difference between peripheral and trunk temperature. The compliance with regard to the intervention was monitored by checking charts, which the mothers maintained. In addition, in the oil massage group the consumption of the oil was also used as a parameter. All infants received measured amounts of expressed breast milk by either gavage or spoon during the study to ensure similar volume intakes. Data collection Baseline characteristics were obtained including birth weight, gestation, sex, Apgar scores, maternal education and socioeconomic status (Kuppuswamy scale)(3). Weight, crown heel length and occipitofrontal head circumference were measured using standard techniques, at enrolment and then weekly for next four weeks. Triceps skin fold thickness was measured in left arm using Holtan’s calipers. Serum triglyceride levels were measured at enrolment and after 28 days of intervention, using the kit "Triglyceride-GPO Reagent Set" (TECO DIAGNOSTICS, California, USA). It is a specific method and makes use of enzymatic hydrolysis and quantification by measuring absorbance at 520 nm. Brazelton’s Neurobehavior Scoring(1) was carried out at enrolment and repeated again ten days after enrolment. The supplementary items specifically meant for preterms were also scored in the recommended manner. For the purpose of analysis, the items were grouped as recommended by Lester(1), with modifications to include the supplementary items for preterms. Statistical Analysis Group means of continuous normally distributed data were compared using analysis of variance (ANOVA). Non-parametric data were analysed using Mann-Whitney U test. Proportions were compared by Chi-square or Fischer exact test. A probability of 5% was considered as significant. Bartlett’s test for homogeneity was used for normality of distribution. Results The study was conducted between March to December 2001. Figure 1 gives the profile of the study and details of inclusion, exclusion and reasons for non-compliance. Table I shows the baseline characteristics of the three groups. The groups were comparable in birth weights, gestation, intra-uterine growth retardation, ponderal index, age at enrolment and enteral feeding patterns.
Out of the sixty-nine infants enrolled, sixty-two (89.8%) completed the trial. Six infants had temporary interruptions in the intervention - 4 in the oil massage group due to apnea, sepsis and IVH; and 2 in the massage group due to apneas. The duration of interruption was significant in three infants in the oil massage group in whom it was >20% of planned massages. Ten other infants had minor problems during the trial (3 in oil massage, 2 in massage and 5 in no massage groups) that neither affected their feeding nor required any interruption in the trial. These problems included oral thrush, pyoderma and hyperbilirubinemia. The baseline characteristics of the infants not completing the trial were comparable to the original group. TABLE I
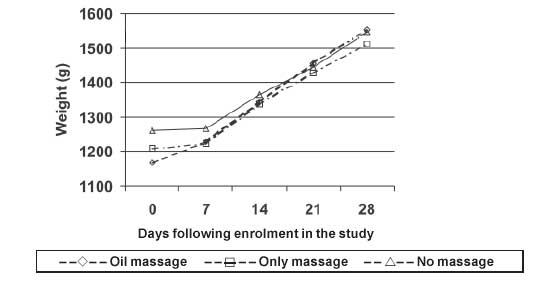
Figure 2 shows the average weights of the infants in the three groups recorded weekly over a period of 4 weeks. Table II shows the anthropometry in the three groups. The mean (SD) weight gain (in grams) over 28 days in the three groups was 365.8 (165.2), 290.0 (150.2) and 285.0 (170.4) in the oil massage, only massage and no massage groups respectively. The weight gain was greater in the oil massage group compared to the other two groups, but they were not significant. In order to adjust for the differences in weight of subjects at the time of enrolment, transforming the weight gain as weight gain/kg/day (g/kg/day), standardized the increment in weight. The adjusted weight gain was more in the oil massage group compared to the other two groups, but the differences were not statistically significant. However, it was observed that infants who had >20% of their scheduled massages interrupted, it resulted in either no weight gain or a loss in weight during the period of interruption. There were three infants who had more than 20% interruption in their massage and all were in the oil massage group. When the adjusted weight gain was analysed after exclusion of these three infants, it was observed that the weight gain in the oil massage group (11.6 + 4.3 g/k/d, n = 17) was significantly greater than in the only massage or no massage groups.
Table II
The overall increment over 28 days in length, head circumference and triceps skinfold thickness was more in the oil massage group compared to the other two groups though it was statistically insignificant. The mean (SD) initial levels of S. triglycerides in the three groups were 129.6 (67.5) mg/dL in the oil massage group, 122.1 (36.6) mg/dL in the only massage group and 136.2 (62.2) mg/dL in the no massage group. The values at 28 days were 127.2 (57.6), 130.2 (47.2) and 134.9 (61.3) mg/dL in the oil massage, only massage and no massage groups respectively. The differences were insignificant. Neonatal Behavior Assessment Scores were summarised according to the seven-cluster scoring method(1). Table III compares the initial and final scores of the three groups in all the seven clusters. No significant difference was found among the three groups either at enrolment or at 10 days in any of the items. TABLE III Neonatal Behavior Assessment Score (Mean, SD).
Discussion The benefit of massaging preterm neonates with or without oil on their growth has remained unresolved, as both these interventions have never been studied together in a controlled trial. The present study, therefore, attempts to resolve this issue through a randomised controlled trial. Soriano, et al.(4) in a trial of 60 preterm neonates reported significantly higher weight gain over a 30 days period in the oil massage group compared to those who received routine care (703 + 129 g vs 576 + 140 g; P <0.05). Field(5) in a review of supplemental stimulation of preterm neonates has identified 23 studies. However amongst them there were only two controlled trials that had used only tactile stimulation as an intervention. Each of these studies enrolled 48 subjects. Both had reported greater weight gain in infants receiving stimulation compared to controls after a 10-day intervention period. Solkoff, et al.(6), failed to document any significant difference in weight gain as a result of massage over 10 days. This study however had a sample of only 16 neonates. In the present trial, a higher weight gain over twenty eight days was observed in the oil massage group compared to only massage or no massage groups with the study powered at 0.7. A slightly larger sample of about 20 more subjects would have had adequate power to detect a significant difference. Also, the differences in weight gain between the only massage group and the controls were insignificant. In the present study, the standardized weight gain, after excluding infants who had >20% of massage interruption, was significantly greater in the oil massage group (11.6 + 4.3 g/kg/day) as compared to only massage group (8.7 + 4.6 g/kg/day) and no massage group (8.3 + 4.9 g/kg/day). Dabi, et al.(7) also reported a significantly higher standardized weight gain in the oil massage group (19.18 + 4.38 g/kg/day) compared to the control group (14.25 + 3.92 g/kg/day). The reported weight gain in the present study was lower than that of Dabi’s trial, possibly because the present trial had a large proportion (>80 %) of growth retarded babies. The data of the present study indicates that the improved weight gain was probably due to oil absorption as the weight gain in the only massage group was no different from controls. The mechanism by which cutaneous application of oil improves weight gain is unclear. The early trials on use of cutaneous application of oil for reversal of essential fatty acid deficiency in neonates receiving total parenteral nutrition have documented its absorption and beneficial effect(8). In the present study since serum triglyceride levels were not altered by cutaneous oil application, it can only be hypothesized that the absorbed oil is possibly stored in the fat cells without significantly altering body fat metabolism. It acted as a source of energy and nutrients and improved overall growth. Soriano, et al.(4) demonstrated a significant increment in length, triceps skinfold thickness and mid arm circumference after 30 days of oil massage in preterm neonates. However, the present study failed to demonstrate any significant change in these anthropometric parameters, though they were more in the oil massage group than in the other two groups. Earlier trials have suggested that tactile and kinaesthetic stimulation could have beneficial effect on preterm neurobehavior. The only trial that evaluated the effect of tactile stimulation using Brazelton’s neuro-behavior scoring was that by Solkoff, et al.(6) which demonstrated the beneficial role of massage in improving neurobehavior of preterm babies. A difference of >2 points in many parameters like habituation and motor maturity was shown after 10 days of stimulation. However, the present study using the same scale (NBAS)(1) could not demonstrate significant improvement in any of the clusters after intervention. In conclusion, it may be stated that oil application may have a potential to improve weight gain among preterm very low birth weight neonates. Since this is a culturally accepted practice, it should be encouraged as a part of the overall package of early neonatal intervention in very low birth weight infant care both in hospitals and at home. However, separate analysis of babies with appropriate and retarded intra uterine growth could not be done because of inadequate sample size. Whether growth retarded and appropriately grown babies benefit equally from oil massage needs to be further evaluated. Contributors: JA conducted the study and drafted the manuscript. Both AK and SR designed and monitored the study, reviewed and edited the manuscript. SR analyzed the data and will act as the guarantor of the study. Funding: None. Competing interests: None stated.
| ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
References | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
| ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
![]()