|
|
Editorial Indian Pediatrics 2005; 42:1081-1085 |
||
|
Novel Therapies Need Full Outcome Assessments |
||
|
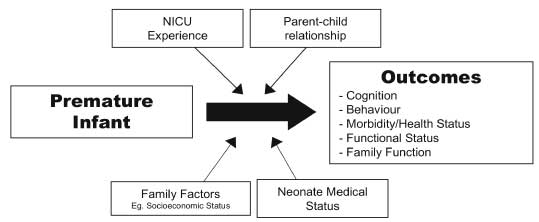
This issue of Indian Pediatrics contains articles on some novel therapeutic approaches in the Neonatal Intensive Care Unit (NICU). Fully assessing new therapies in this population is very relevant to India, since over 20 million infants worldwide are born with low birthweight (<2500 g), of which 96% are born in developing countries(1). Although innovations in the NICU have dramatically increased survival among premature infants, there has not been a concomitant decrease in morbidity. The prevalence of disability in survivors, such as cerebral palsy, broncho-pulmonary dysplasia, blindness, deafness, and deficits in cognitive and behavioural development, remain of concern. For example, the EPI-CURE study assessed 241 children (78% of survivors) at school age who were born at less than 26 weeks. In comparison to a control group of 160 full term classmates, 41% of extremely preterm children versus 2% in the control group were found to have cognitive impairment(2). Choosing outcomes to measure and ensure validity Full assessment of new therapies, entails sensible choice of a primary outcome, that is biologically credible, clinically important and potentially responsive to the intervention(3). The timing of outcome assessment should account for possible intervention effects on later growth and development(3). One should ask if the outcome measures of a trial, adequately reflect the long-term development status of preterms. For example, prior trials of indomethacin prophylaxis in newborns had shown the reduction in serious intraventricular hemorrhage. Biological plausibility suggested clinical significance, but it was unclear whether this translated into an enduring effect. A large (n = 1202) multicenter trial (Trial of Indomethacin Prophylaxis in Preterms), found that while one quarter of surviving extremely low birth weight infants had moderate-to-severe cognitive delay at 18 months corrected age, indomethacin prophylaxis did not play any role in reducing this burden(4). The difficulty with a long term study is obviously the additional cost and trouble entailed. But unless near to complete follow up is ensured, bias may be introduced. This is of great importance, as preterm infants who are followed with ease may not have the same outcomes as those who are followed with difficulty. Tin, et al. found a lower general developmental quotient in children whose families were reluctant for assessment(5). Finally, a blinded assessment of follow-up could be viewed as a welcome opportunity to allow for correction of the bias introduced by an inability to blind the initial intervention. Etiological pathways Clinicians providing evidence-based estimates of potential impairments for preterm infants are hampered by uncertainty in the etiological pathway. Concretely, the impact of premature birth may be mediated by the neonate’s medical status, family factors, the NICU experience, and the parent-child relationship (Fig. 1)(6).
Certainly, disadvantage may result from physiological insults. A simple count of three common neonatal morbidities; broncho-pulmonary dysplasia, brain injury and severe retinopathy of prematurity, predict neurosensory impairment(7). However, less obvious aetiological pathways may be present. For example, the sensory impact of the NICU environment and its "neuro-overload" also impact development, and a group of interventions termed ‘developmental care’ were designed in response(8). But other important influences include family factors such as age, ethnicity, socioeconomic (SES) status, employment, family configuration, level of social support, and education, which can also themselves lead to preterm birth(9,10). Poverty does not only increase the risk of preterm birth, it also reduces the probability that a preterm survivor will be provided an optimal environment. A recent study of preterm infants followed to age 10 found that family factors were stronger predictors of school performance than perinatal complications(11). This highlights the role of parent-infant interactions, which may be compromised for premature infants for several reasons including: parents emotional responses to premature birth, changes in the parental role and the infant’s characteristics. Parents may not have "learnt" to interact normally with the fragile, sick, hospitalized preterm resulting in an impaired relationship with the premature infant, which may place these infants at risk for adverse developmental outcomes. Thus outcomes of preterm birth may reflect the interplay of biological and environ- mental factors. It is for this reason that "unconventional therapies" such as massage, are important to evaluate. Massage therapy has a biological plausibility since sensory input might modify inappropriate ‘neuro-overloads’ while promoting care-giver (parental) interaction with the newborn. Early interventions–massage therapy Massage therapy is one of several early intervention programs used to promote growth and development in preterms. Massage is a traditional practice in the African and Asian continents, and has gained popularity in NICU’s of the western world. However, a recent Cochrane systematic review of massage therapy for preterm infants concluded that due to methodological limitations, only weak evidence suggests that massage benefits developmental outcomes(12). Moreover, the review indicated that massage may improve daily weight gain by an average of 5 g, although the pooled results also showed a reduction in the length of NICU stay by 4.6 days. The two trials reported in this and an earlier(13,14) issue accord with the results of other trials that found beneficial effects of massage on weight gain(12). The primary outcome for most massage interventions has been weight gain approximately thirty days after enrolment in the study. Also, most studies were small and powered to detect a weight gain of around 3 g/kg/day, and thus may not have had adequate power to detect a difference of clinical importance. Clinicians assessing these papers, need to assess whether these changes are not only statistically significant, but also of clinical significance. Few massage therapy studies assessed outcomes after the intervention period finished, leave aside into early childhood. Some trials assessed acute neurodevelopmental results from the Brazleton Neonatal Behavioral Assessment Scale (n = 4), or assessed later outcomes by the Bayley Scale, largely before 9 months (n =3)(12). However, the predictive ability of the Brazelton with regards to later intellectual functioning is not clear. Moreover, the later the Bayley test is given (i.e., beyond 24 months) the more predictive it is for later childhood functioning(16). Finally, numerous studies did not demonstrate complete follow up. Other early interventions involving parents Massage may not have any specific biological role, but may function as a surrogate for improving the parent-infant relationship. Premature birth has a strong impact on parents as well as the preterm infant. Parents experience psychological distress, such as anxiety, depression, disappointment, guilt, helplessness, fear, and loss of control after the birth of a preterm infant(9,17). These emotions combined with the NICU environment, prolonged parent-infant separation and the premature infants characteristics, alter the expected parental role, and may influence parental behavior. Studies of parents of preterm infants one year post birth, found that mothers were less responsive to their infants, provided a less stimulating environment, and gave less positive feedback than mothers of term infants(17-20). The quality of the parent-infant relation-ship is essential for building a solid foundation for a child’s development. Thus the impact of premature birth on the parent-infant relationship ultimately may exacerbate the risk of these children for impairments. This emphasizes the need for interventions that improve parent-infant interactions. Infant massage is one potential intervention that can be used to promote the parent-infant relationship. Teaching parents to massage their infants may build on parent’s strengths and empower them in caring for their infant. It may also allow them to feel included in the NICU setting and teach them about their infant’s characteristics. A study of mothers with postnatal depression found that infant massage enhanced bonding with their child and increased confidence in parenting skills(21). We have conducted a systematic review of intervention programs that either taught parents skills and/or involved them in aspects of care for their infant (ESPR, 2005). Our primary outcome of interest was neurodevelopment at 12 and 24 months corrected age. We included randomized controlled trials from 1966 to 2004 of premature infants that conducted an intervention in the first 12 months of the infant’s life, as compared to routine care/non-intervention controls. Meta-analysis of neurodevelopmental outcomes, as measured by the mental (MDI) developmental indexes of the Bayley scale found a pool weighted mean difference of greater than 7 points (P < 0.01) between the MDI scores of the intervention and control groups. These finding suggest that positive results arise for interventions that enhance the parent-child relationship, which may help decrease or prevent impairments for preterm survivors. Conclusion More studies are required that identify effective interventions in order to improve the long-term outcomes of this vulnerable population and their families. While the challenges of designing, funding and carrying out such trials appear daunting, the need remains clear. It is not only the neonatal specialists who should be interested in these questions, since the survivors of the NICU become the later challenges of the Pediatric community and ultimately, of society. Funding: None. Competing interests: None. Haresh Kirpalani,
| ||
|
![]()