|
|
Case Reports Indian Pediatrics 2002; 39:1044-1047 |
||
|
Giant Solitary Parathyroid Adenoma Presenting with Bone Disease |
||
|
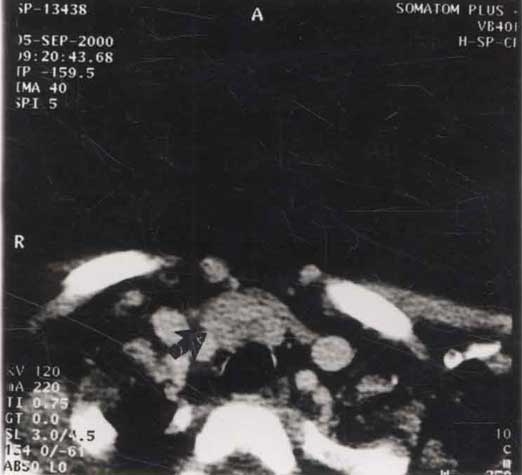
Primary hyperparathyroidism, most common in adults in the fifth and sixth decades of life, is unusual in children. The most common cause is a solitary parathyroid adenoma. Parathyroid adenomas are benign tumors, may be extremely small and can occur in ectopic sites, being difficult to locate even at surgical exploration. Successful neck exploration and excision of the adenoma is associated with reversal of lesions and symptomatic improvement. Case Report A 12 year old girl presented with complaints of obesity, inability to walk because of neuromuscular weakness and fractures of left wrist and forearm due to trivial trauma. The fracture site showed non union even after closed reduction and immobilization. The patient was wheel chair bound because of increased fatiguability and muscular weakness. She had not attained menarche and there were no associated abdominal colic, neuropsychiatric distur-bances or hypertension. She had a palpable lump in the lower part of the neck measuring 3 × 2 cm. With a clinical supsicion of hyperparathyroidism, the investigations revealed hypercalcemia (serum calcium 12 mg/dL), hypercalciuria (24 hr urine calcium 6.0 mg/kg/day; normal range 4.2-5.4), elevated serum alkaline phosphatase (2533 IU; normal range 105-420) and hyperparathyroidism (PTH 1949 pg/mL; normal range 1-43). The thyroid function tests were normal. An ultrasound and CT scan of the neck revealed a large parathyroid adenoma ( 3 × 2 cm) in the region of the right inferior parathyroid (Fig.1). The skull x-ray showed punched out lesions typically described as salt and pepper appearance. The patient was explored and the right inferior parathyroid adenoma was excised. The other three parathyroid glands were looked for but could not be identified; tissue samples from the possible sites were negative for parathyroid tissue. Following the excision, the parathormone levels dropped precipitously from 1949 pg/mL to 230 pg/mL in 1 hour and were measured as 98 pg/mL 6 days after the procedure; the serum calcium levels had normalized. In the immediate postoperative period the patient developed carpopedal spasms which were relieved by parenteral calcium infusions. Within two weeks postoperatively, the patient showed further symptomatic improvement, did not require parenteral calcium infusions and has become ambulatory without support. The histopathological examination confirmed the diagnosis of parathyroid adenoma, weighing 5.52 g.
Discussion There are few case reports in the literature describing large parathyroid adenomas in children(1,2,3). These are benign tumors, usually very small in size weighing 0.5 - 5 g, although extreme weights of over 100 g have been reported. Tumors weighing more than 5 g are termed, giant parathyroid adenoma. The adenoma size is a major determinant of disease severity and manner of presentation. It has been proposed that vitamin D deficiency prevalent in developing countries contributes to the stimulated growth of parathyroid adenoma. Improved vitamin D nutrition in the population is perhaps responsible for the changes in disease severity and manner of presentation that have occurred over the last five decades(4). For obscure reasons they are usually located in the inferior parathyroid glands. They can occur in ectopic sites such as behind the esophagus, thymus, pericardium or thyroid glands, thus creating problems in surgical exploration. No case of hypercalcemia should be labelled as idiopathic without a detailed exploration of the neck to exclude primary hyperparathyroidism from a parathyroid adenoma(1). Hyperparathyroidism occurs in approximately 25 per 100000 in the general population. The disease is rare in children; there are fewer than 200 reported cases of childhood primary hyperparathyroidism. Parathyroid lesions account for upto 30% of cases of hypercalcemia and although the exact incidence of solitary parathyroid adenoma is not available, they are the cause for hyperparathyroidism in >80%, although parathyroid hyperplasia (15%), double adenomas (2-3%), malignancy (2%) and familial endocrine syndromes may also cause hyperparathyroidism. Parathyroid tumors are virtually benign with an estimated incidence of parathyroid carcinoma causing hyper-parathyroidism in only 0.017% of cases. Virtually all parathyroid neoplasms are functional(5-8). The affected patients present with neuromuscular weakness, easy fatiguability, neuropsychiatric disturbances, renal stones, gallstones, osteitis fibrosa cystica, hypertension, pancreatitis, peptic ulcer and metastatic calcification. Osteopenia is an important feature of primary hyperparathyroidism(7). The radiological studies have revealed sub-periosteal bone resorption, cortical atrophy of long bones, cysts, brown tumors and soft tissue calcification(8). Quantitative computed tomography has shown that the catabolic effect of parathormone on cortical bone in the form of osteoclastic resorption may be associated with a simultaneous anabolic effect on cancellous bone giving rise to osteosclerosis. Parathormone may cause a significant redistribution of the bone mineral from cortical to cancellous bone. After parathyroidectomy the cortical and cancellous bone density value increases with the decrease in the serum concentrations of calcium and to a lesser extent phosphorous, due to the hungry bone syndrome. The major increase in bone mineral density occurs within three months following parathyroidectomy(9). The lesions described are usually not seen now a days because of increased awareness of the disease and early diagnosis. Elevated serum alkaline phosphatase is found to be associated with parathyroid adenoma and hyperparathyroidism as seen with our patient(3,10). With daily follow up of serum parathyroid hormone and calcium after parathyroidectomy, it has been shown that the first day’s parathormone level is a reliable indicator of the success of parathyro-idectomy(11). An increased incidence of parathyroid adenoma has been noticed in children who received radiotherapy for orbits, lungs or thyroid. Routine monitoring of serum calcium and phosphate levels is recommended for children after head and neck irradiation(12). Contributors: VB was the principal surgeon and TRSP was the assistant. The literature search and manuscript preparation was done jointly. Funding: None. Competing interests: None stated.
| ||
|
References | ||
|
![]()