The latest guidelines on neonatal resuscitation
from American Heart Association (AHA) [1] and European Resuscitation
Council (ERC) [2] were released in October 2015. There have been slight
variations between these guidelines; although they use nearly identical
literature for evidence evaluation. We present here the major changes in
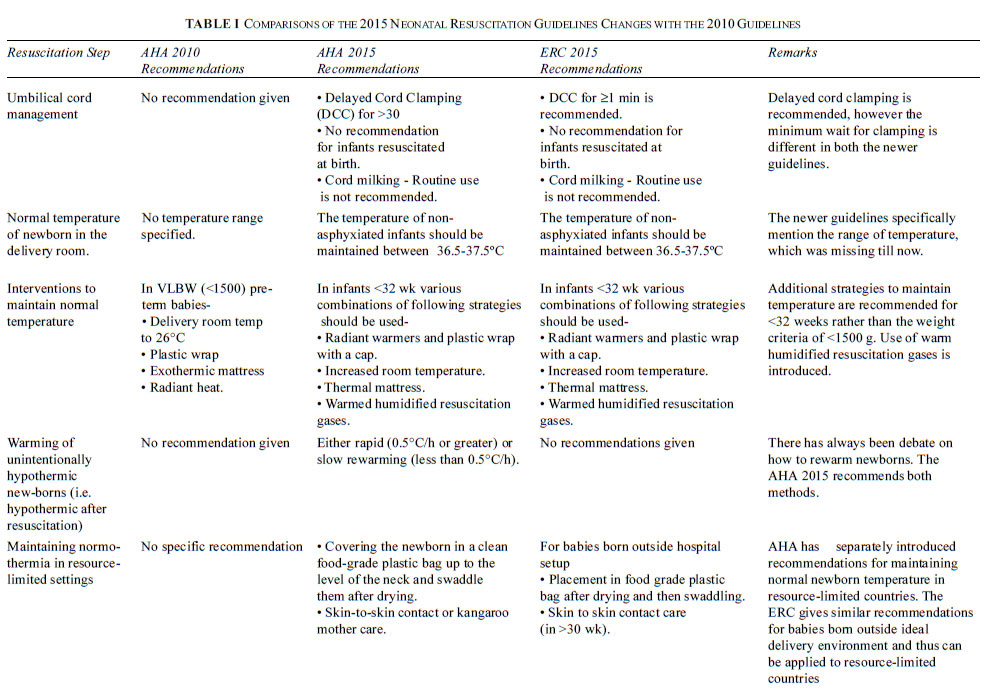
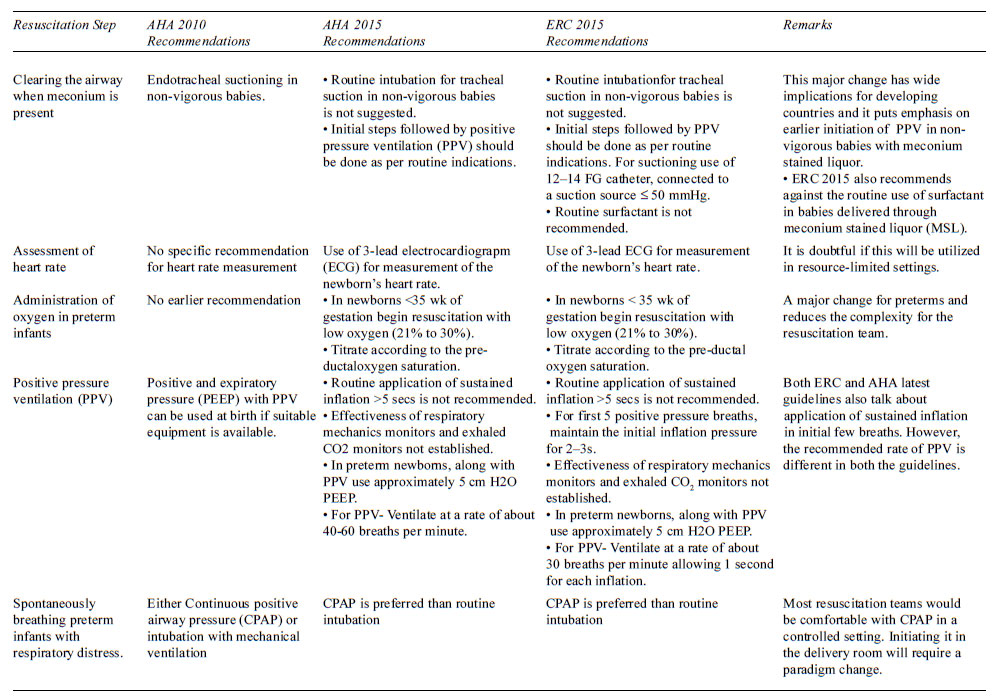
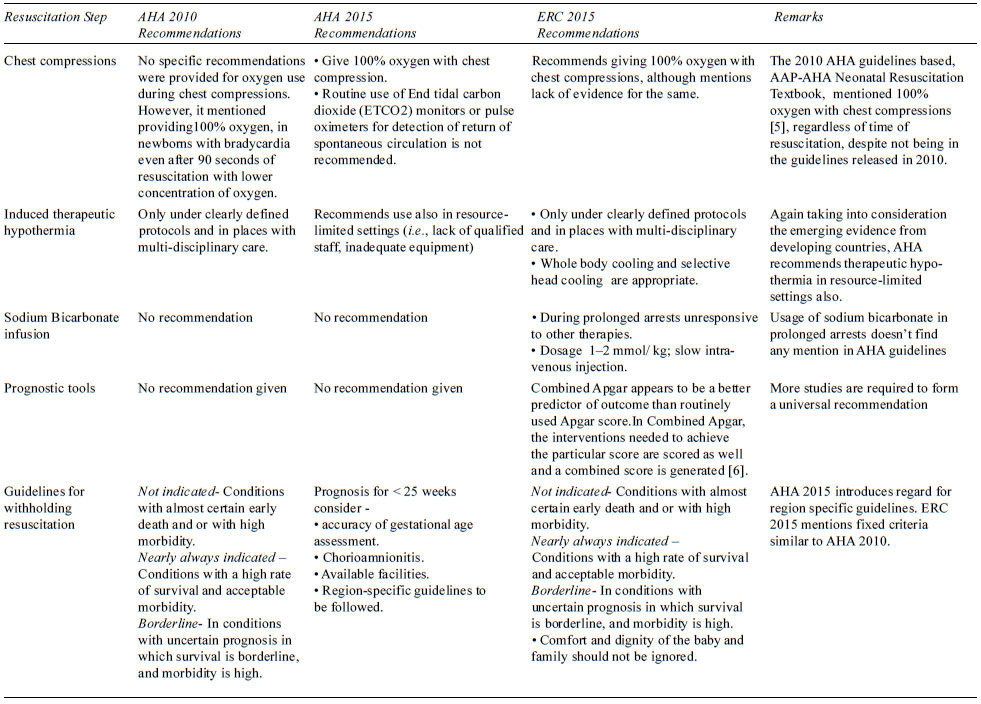
the recent guidelines [3,4], and comparison between the ERC and AHA
guidelines of 2015. The major changes are detailed in Table I.
Some of the major recommendations of previous AHA guidelines are
continued without reviews and are elaborated in Table II.
The major recommendations are summarized in Box 1.
TABLE II Recommendations That Remain Unchanged
|
Temperature control
|
Resuscitation should be performed with temperature-controlling
interventions. |
|
Clearing the airway when amniotic fluid is clear
|
Routine suctioning is not recommended. |
|
Assessment of need of oxygen therapy
|
Oximetry should be used to monitor if any neonate needs
PPV, with persistent and monitoring of oxygen therapy central
cyanosis persists and with the use of supplementary oxygen. |
|
Administration of oxygen in term infants
|
Initiate resuscitation with room air. Supplementary oxygen may
be administered to achieve appropriate pre-ductal oxygen
saturation.
|
|
Initial breaths and assisted ventilation
|
An initial inflation pressure of 20 cm water is adequate; some
term babies may require up to ³30 to 40 cm water. Rate of giving
PPV- 40 to 60 per minute. |
|
Endotracheal tube placement
|
Exhaled CO2 detection is most reliable. |
|
Chest compressions
|
Coordinated chest compressions and PPV should be done if heart
rate<60 per minute after establishing effective ventilation.
|
|
Epinephrine
|
IV dose - 0.01 to 0.03 mg/kg of 1:10 000 epinephrine. For an
endotracheal route - 0.05 to 0.1 mg/kg.
|
|
Volume expansion
|
Volume expansion when blood loss is known/suspected.Dose - 10 mL/kg
of isotonic crystalloid solution or blood, may be repeated.
|
Implications for Resource-limited Settings
With the emergence of scientific evidence from
developing countries, these studies from resource-limited countries are
forming the basis of major changes in clinical practice guidelines.
Also, specific and separate recommendations are being made for
resource-limited settings, as many of the standard recommendations may
not be feasible in these settings.
We discuss some of the points below to put things
into perspective:
• Therapeutic hypothermia has been recommended in
resource-limited setups. The cost is still forbidding for those in
need as well as the availability of centers that can provide it.
Newer phase-change material based devices are available and evidence
is increasing of its safety for use in Indian conditions [7].
• Skin-to-skin contact has been stressed as a
method for maintaining newborn temperature in the peri-partum period
based on evidence drawn from India and other resource-limited
countries [8].
• The evidence for delayed cord clamping has
grown stronger as well as the evidence for cord milking. The
guidelines caution against cord milking below 29 weeks. This has
great relevance to neonatal management and is a significant change.
• Removal of routine tracheal suction in
non-vigorous neonates is a welcome change, leading to uniformity of
the guidelines in all the scenarios. This significant change is
contributed by evidence drawn from India [9].
• The routine use of ECG and pulse oximeters,
might find little practical use in resource— limited settings. There
is still no data available of widespread use of pulse oximeters in
India and given the resource constraints this change may not be
practiced uniformly.
• Similarly, use of exhaled CO
monitors, oxygen blenders, and laryngeal mask airways will remain
out of reach in most resuscitation situations in resource limited
settings
• Decreased usage of oxygen in preterm newborns,
and preference CPAP over mechanical ventilation might contribute to
the decentralization of newborn care and better care at level 1 or
level 2 setups.
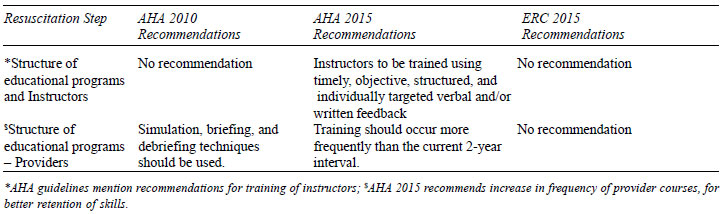
• While earlier there was a mandate for training
all health personnel involved in neonatal care every two years in
neonatal resuscitation, the committees have recommended more
frequent trainings without stipulating, a duration between
trainings. The evidence is rising for ‘Low Dose High Frequency’
trainings for neonatal resuscitation.
Conclusion
There are critical changes in updated resuscitation
guidelines of 2015 with subtle differences between the AHA and ERC. The
authors believe that the Indian Academy of Pediatrics and the National
Neonatology Forum of India will bring out India-specific recommendations
to guide the resuscitation methods to be followed in India. This will
ensure that the clinicians practicing resuscitation on a daily basis
have some basis for their variance from International Guidelines.
1. Wyckoff MH, Aziz K, Escobedo MB, Kapadia VS,
Kattwinkel J, Perlman JM, et al. Part 13: Neonatal Resuscitation:
2015 American Heart Association Guidelines Update for Cardiopulmonary
Resuscitation and Emergency Cardiovascular Care. Circulation.
2015;132:S543-60.
2. Wyllie J, Bruinenberg J, Roehr CC, Rüdiger M,
Trevisanuto D, Urlesberger B. European Resuscitation Council Guidelines
for Resuscitation 2015. Resuscitation. 2015;95:249-63.
3. Kattwinkel J, Perlman JM, Aziz K, Colby C,
Fairchild K, Gallagher J, et al. Neonatal Resuscitation: 2010
American Heart Association Guidelines for Cardiopulmonary Resuscitation
and Emergency Cardiovascular Care. Pediatrics. 2010;126:e1400-13.
4. Roehr CC, Hansmann G, Hoehn T, Bührer C. The 2010
Guidelines on Neonatal Resuscitation (AHA, ERC, ILCOR): similarities and
differences—what progress has been made since 2005? Klin Padiatr.
2011;223:299-307.
5. Kattwinkel J, ed. Textbook of Neonatal
Resuscitation. 6th ed. Elk Grove Village, IL: American Academy of
Pediatrics, American Heart Association, 2010. p.146
6. Dalili H, Nili F, Sheikh M, Hardani AK, Shariat M,
Nayeri F. Comparison of the four proposed Apgar scoring systems in the
assessment of birth asphyxia and adverse early neurologic outcomes. PloS
One. 2015;10:e0122116.
7. Thomas N, Chakrapani Y, Rebekah G, Kareti K,
Devasahayam S. Phase changing material: an alternative method for
cooling babies with hypoxic ischaemic encephalopathy. Neonatology.
2015;107:266-70.
8. Nimbalkar SM, Patel VK, Patel DV, Nimbalkar AS,
Sethi A, Phatak A. Effect of early skin-to-skin contact following normal
delivery on incidence of hypothermia in neonates more than 1800 g:
randomized control trial. J Perinatol. 2014;34:364-8.
9. Chettri S, Adhisivam B, Bhat BV. Endotracheal
suction for nonvigorous neonates born through meconium stained amniotic
fluid: a randomized controlled trial. J Pediatr 2015;166:1208-13.