|
|
|
Indian Pediatr 2015;52: 439 |
 |
Tetrasomy X in a Child with Upper Limb
Deformity
|
|
Seema Korgaonkar and *Babu Rao Vundinti
National Institute of Immunohaematology (ICMR), KEM
Hospital campus, Parel, Mumbai, India.
Email:
*[email protected]
|
|
49, XXXXY syndrome is a rare sex chromosome aneuploidy in humans with an
incidence of 1:85000 male births [1]. Various clinical features such as
low birth weight, slow growth with reduced bone age, mental retardation,
radioulnar synostosis, multiple skeletal deformities with joint laxity,
clinodactyly, cardiac deformity, abnormal genitals, hypogonadotropic
hypogonadism, and craniofacial anomalies have been reported previously
[2,3]. A 16-months-old male child, born to non-consanguineous parents,
was referred to our laboratory for chromosomal analysis. The mother’s
age was 22 years and father was 35-years-old. The child had dysmorphic
features (hypertelorism, upward slanting eyes, broad nose, low set small
ears with tags, flat occiput), hypoplastic nipples, bilateral
clinodactyly, cubitus varus (deformity in both elbows), flat feet,
delayed dentition, and global developmental delay. Ultrasonography (USG)
of abdomen revealed enlarged spleen and both the kidneys were normal.
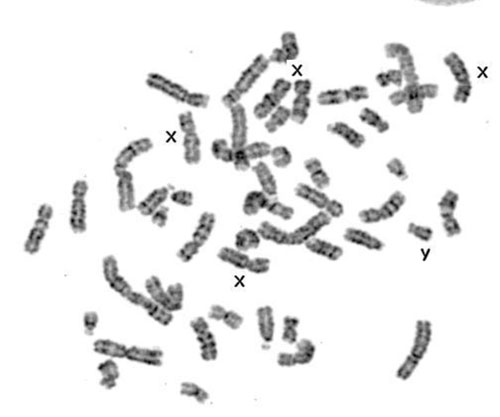
2-D echocardiogram was normal. Cytogenetic analysis of G- banded
metaphases from PHA-stimulated peripheral blood revealed 49, XXXXY
karyotype (Fig. 1). Fluorescence in situ hybridization
(FISH) using centromeric probes of X and Y confirmed tetrasomy X, and
there was no indication of mosaicism.
 |
|
Fig.1. Metaphase showing
tetrasomy X and Y.
|
Tetrasomy X occurs due to two non-disjunction events
in maternal meiosis. Spectrum of clinical features have been reported in
49, XXXXY syndrome [2-4]. The clinical diagnosis of tetrasomy X in
newborns is challenging. Chromosomal analysis plays an important role in
accurate diagnosis. The phenotypic presentation in elderly patients with
tetrasomy X is not known. Follow-up studies are essential in such rare
cases to establish genotype-phenotype correlation. However, the
additional X chromosomes and presence of Y chromosome may influence the
development of Klinefelter syndrome phenotype in tetrasomy X syndrome.
Genetic counselling for the parents is essential for the future
pregnancies.
References
1. Kleczkowska A, Fryns JP, Van den Berghe H.
X-chromosome polysomy in the male. The Leuven experience 1966-1987.
Human Genet. 1988;80:16-22.
2. Fraccaro M, Kaijser K, Lindsten J. A child with 49
chromosomes. Lancet. 1960;22:899- 902.
3. Sijmons RH, van Essen AJ, Visser JD, Iprenburg M, Nelck
GF, Vos-Bender ML, et al. Congenital knee dislocation in a 49,
XXXXY boy. J Med Genet 1995;32:309-11.
4. Kidszun A, Fuchs AJ, Russo A, Bartsch M, Frey-Mahn
G, Beyer V, et al. Skeletal abnormalities of the upper limbs - Neonatal
diagnosis of 49,XXXXY syndrome. Gene. 2012;508:117-20.
|
|
|
 |
|
