|
|
|
Indian Pediatr 2011;48: 390-392 |
 |
Behavioral Response to Pain in
Drowsy and Sleeping Neonates: A Randomized Control Study |
|
Sheila S Mathai, Amit Naresh and Sathyajit Sahu
From INHS Asvini (Naval Hospital), Colaba, Mumbai, India.
Correspondence to: Dr Sheila S Mathai, Professor and Head
of Department (Pediatrics), INHS Asvini (Naval Hospital), Colaba, Mumbai
400 005, India.
Email: sheilamathai@yahoo.com
Received: May 24, 2010;
Initial review: September 8, 2010;
Accepted: September 15, 2010.
Published online 2011 Feb 28.
PII: S097475591000430-2
|
|
Abstract
In a randomized controlled design, 100 healthy, term
neonates in the first week of life, undergoing heel prick for routine
screening were randomized to receive a heel prick in either the
drowsy/sleeping state or the awake (but not fussy or crying) state. 48
babies in sleeping or drowsy states and 47 in the awake states were
analyzed. Infants in the drowsy/sleeping states scored significantly
lower on the Neonatal Infant Pain Score (NIPS) (median score 5) at 30
seconds post stimulus compared with infants in higher states of
alertness (median score 6). They also had a shorter total duration of
cry (29.17sec ± 8.95 vs 32.67 sec ± 9.82). However, there was no
difference in the NIPS score between the two groups at 45 seconds post
stimulus. We concluded that babies in the drowsy/sleeping states of
alertness at the time of a painful stimulus appear to show a less
intense behavioral response to pain as compared to those in the awake
state.
Key words: Neonate, Pain, Response, Sleep.
|
|
Most pain scores commonly used in neonates do not take into
consideration the state of alertness of the baby at the time of the
painful stimulation and, if they do, they do not score an awake or
sleeping state prior to stimulus differently [1]. Though there are a few
studies that suggest that babies who are more alert manifest a more robust
response to pain, these findings are not definite enough to make
recommendations [2]. This study was carried out to determine if the
initial state of alertness at the time of the noxious stimulus made a
significant difference to the behavioral response to the pain of a heel
prick in healthy, term neonates.
Methods
One hundred healthy, term, appropriate for gestation
age neonates, undergoing heel prick for newborn screening, were enrolled
during the first week of life. All neonates were on breastfeeds and not on
any medication or phototherapy. Infants less than 2000 grams, those with
inherent neurological problems, those who had suffered birth asphyxia or
had major congenital anomalies were excluded.
The sample size was based on the assumption that
neonates would score between 3 and 7 on Neonatal Infant Pain Scale (NIPS)
scores during a heel prick. To demonstrate a difference in the pain scores
of at least 20% with a significance level of 5% and power of 80%, the
sample size was calculated to be at least 45 in each of the two study
groups. Hospital Ethics Committee approval was taken to conduct the study.
Informed consent was taken from parents.
Simple randomization was done by random number tables
and allocation was concealed by numbered envelopes. Neonates were
randomized to receive the heel prick in either the awake or the
asleep/drowsy state of alertness.
In Group A, heel prick was administered in
drowsy/sleeping states of alertness (Brazelton States 1, 2 and 3) [3].
These states were determined to be present if the infants’ eyes were
completely or partially closed and there was no significant limb movement
when unwrapped. In Group B, heel prick was administered in the quiet
alert/active alert states of alertness (Brazelton States 4 and 5). These
states was determined to be present if the infant’s eyes were definitely
open and there were at least some limb movement when unwrapped but the
baby was not fussy or crying.
 |
 |
|
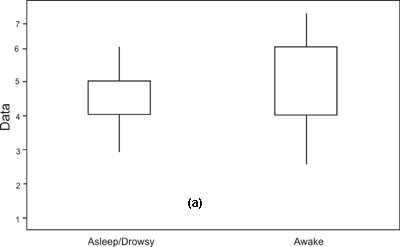
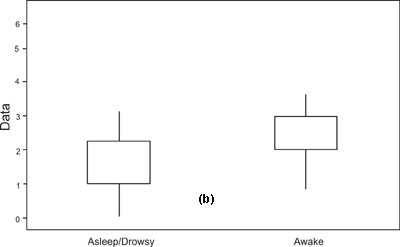
Fig. 1 Box and
Whisker plots showing difference between pain scores at (a) 30s and
(b) 45s after stimulus in the two groups. |
Each neonate was tested for response to pain by two
observers. After unwrapping and gently cleaning the heel but before
administering the painful stimulus, the first observer ensured that the
neonate was in the correct state of alertness of the group allotted.
Baseline scoring on Neonatal Infant Pain Scale (NIPS) [4] was done by this
observer who then also administered the heel prick. This was done with a
standard lancet so that a 3-4 mm drop of blood was visible on the skin
without squeezing. If the blood was inadequate it was assumed that the
heel prick was not deep enough and the test was abandoned. No infant was
pricked twice. If the infant was not in the correct state of alertness
within 30 minutes of being randomized, the test was abandoned. The first
observer also noted the duration of cry with the help of a stopwatch. The
time from the start of the cry to the first inspiration (first phase of
cry) and total duration of crying were both recorded. The second observer,
who was blinded to the group assignment, stood behind a screen till the
heel prick was given. He then entered the test area and did the pain
scoring at 30 and 45 seconds. Validity of measurement and internal
consistency was done by randomly video-recording 10% of cases and
rescoring by the same observers. Parametric data were recorded as mean and
SD and Student’s t test was used for comparison. Pain scores were
analyzed as non-parametric data and medians were compared by Mann Whitney
test.
Results
After randomization, 5 children were excluded from
analysis as they could not be tested satisfactorily due to various reasons
including inability to get the baby into the correct state of alertness (3
cases) and inability give a deep enough heel prick to get an adequate
sample (2 cases). Finally, 95 babies were analyzed (Group A: 48; Group B:
47).The two groups were equally matched in demographic parameters except
that there were more boys than girls in the awake group (Table I).
TABLE I
Demographic Data of Study Group
|
Parameters |
Asleep /Drowsy |
Awake |
| |
(n = 48) |
(n = 47) |
|
Male: Female |
1.04:1 |
1.23:1 |
|
Birth weight (kg),* |
2.93 (0.35) |
2.92 (0.46) |
|
Gestational age (wks),* |
38.65 (1.06) |
38.83 (1.04) |
|
Age at study (hrs),* |
46.33 (35.67) |
38.39 (34.86) |
|
Time from last feed (min),* |
31.56 (24.19) |
26.85 (30.58) |
|
Type of delivery (vaginal/LSCS) |
33/15 |
34/13 |
|
* Values in mean (SD) |
Awake infants (Group B) had higher median NIPS scores
than Group A infants immediately before the stimulus (3 vs 2) and
30 seconds post stimulus (6 vs 5). However, at 45 seconds there was
no difference in the median scores in the two groups (2 in both groups).
Total duration of cry was found to be lesser in babies who were asleep or
drowsy at the time of stimulus (29.2±8.95s vs 32.7±9.82s). How-ever
the duration of first phase of cry (time from onset of cry to the first
inspiration) was longer in sleeping or drowsy babies as compared to awake
infants (4.1±1.24s vs 2.9±1.18s).
Discussion
It has been observed that the state of alertness at the
time of a painful stimulus may affect pain scores in neonates. A few
studies have shown that more highly aroused, awake infants appear to
respond more intensely to pain as compared with sleepy infants [5, 6]. The
NIPS score is one of the few scores that takes the state of alertness of
the baby into consideration The baby is scored 0 if he is either asleep or
awake and 1 if he is ‘fussy’ Both sleep and awake are scored the same [4].
Some workers have shown that restraining a baby during administration of a
painful stimulus results in a decreased pain score and that handling
infants before a painful stimulus results in infants having a higher score
[7]. However, to date, there are no recommendations regarding
consideration of the state of alertness at the time of the painful
stimulus when assessing pain by behavioral scores. This may lead to
fallacious interpretation of results when assessing the effects of pain
relieving strategies in neonates. Sleepy or drowsy babies may be
interpreted as experiencing less pain as compared to alert ones when
exposed to the same intensity of painful stimulus, This may lead to bias
in the assessment of the effect of interventions for pain [8].
Our study shows that the state of alertness at the time
of the painful stimulus made a significant difference in the behavioral
response to heel-prick in term neonates. This was collaborated by the
duration of cry which was also different in the different states. The
duration of first phase of cry (i.e. from the start of crying to
the first inspiration) which was longer in sleeping or drowsy babies could
suggest irritation at being woken up rather than actual pain.
We recommend that all interventional studies using only
behavioral pain scores should take into consideration the state of
alertness at the time of the painful stimulus, when interpreting pain in
neonates.
Acknowledgment: Mr Ranjan Samanta, BSc
(Economics and Statistics) for statistical analysis of data.
Contributors: SSM conceived and designed the study
and revised the manuscript for important intellectual content. She will
act as guarantor of the study. AN, and SS collected data and assisted in
drafting and analysis. The final manuscript has been approved by all
authors.
Funding: None. Competing interests: None
stated.
|
What This Study Adds?
• Lower states of alertness appear to result in
lower behavioral pain scores in neonates.
|
References
1. Duhn LJ, Medves MJ. Systematic integrative review of
infant pain assessment tools. Adv Neonatal Care. 2004;4:2004.
2. Lawrence J, Alcock D, McGrath P, Kay J, MacMurray
SB, Dulberg C. The development of a tool to assess neonatal pain.Neonatal
Netw. 1993;12:59-66.
3. Brazelton TB, Nugent JK.The Neurobehavioural
Assessment Scale. 3rd Edition. London: MacKeith Press.1995.
4. Lawrence J, Alcock D, McGrath P, Kay J, MacMurray
SB, Dulberg C. The development of a tool to assess neonatal pain. Neonatal
Netw. 1993;12:59-6.
5. Grunau RVE, Craig KD. Pain expression in neonates:
facial action and cry. Pain. 1987; 28:395-410.
6. William AL, Khattak AZ, Garza C, Lasky RE. The
behavioral pain response to heelstick in preterm neonates studied
longitudinally: Description, development, determinants, and components.
Early Human Dev. 2009;85:369-74.
7. Porter FL, Wolf CM, Miller JP. The effect of
handling and immobilization on the response to acute pain in newborn
infants. Pediatrics. 1998;102:1383-9.
8. Weissman A, Aranovitch M, Blaze S, Zimmer EZ.
Heel-lancing in newborns: behavioral and spectral analysis assessment of
pain control measures. Pediatrics. 2009;124:e920-8.
|
|
|
 |
|
