|
|
|
Indian Pediatr 2010;47: 423-428 |
 |
Artemisinin Derivatives Versus
Quinine for Severe Malaria in Children: A
Systematic Review and Meta-Analysis |
|
Joseph L Mathew
From the Advanced Pediatrics
Centre, PGIMER, Chandigarh 160012, India.
Email:
[email protected]
|
|
Relevance
In uncomplicated malaria, the WHO
recommends Artemisinin-based combination therapy
(ACT) (1) for infants and children. However, the
Government of India recommends chloroquine for
P.vivax and also P.falciparum in areas
without resistance; ACT is advised only for
confirmed P.falciparum in 117 districts with
documented chloroquine resistance(2).
In contrast, the treatment of
severe/complicated childhood malaria appears to be
evolving. The 2005 IAP Guideline followed the
National Malaria Programme and recommended quinine,
suggesting artesunate/artemether as less preferred
alternatives(3). In 2008, it was modified as quinine
with tetracycline/doxycycline/clindamycin(4) in line
with the WHO 2006 statement. The National Guideline
2009(2) suggests artesunate, quinine, artemether, in
that order, contraindicating arteether and
doxycycline in children. The WHO’s 2010 Guideline(1)
strongly recommends aresunate in adults with severe
malaria, positioning quinine only as an alternative;
however, it cites lack of evidence to frame a
similar recommendation for children.
Despite appropriate therapy with
parenteral quinine, the case fatality rate in severe
malaria exceeds 20-30%. In addition, quinine
administration requires hospital facilities for
controlled infusion under close monitoring, owing to
the risk of potentially serious (albeit treatable)
side effects. Therefore alternate therapies are
sought, to improve clinical outcomes and also
simplify administration. Artemisinin derivatives
appear to hold promise in this direction.
This systematic review of
evidence addresses the question: "In children with
severe/complicated malaria (population), do
Artemisinin derivatives (intervention),
improve clinical outcome in terms of mortality,
clinical recovery, parasite clearance, adverse
effects, etc (outcome), as compared to
standard parenteral quinine therapy (comparison)?
Current Best Evidence
A Medline search updated on 25
March 2010, with "severe malaria" and Limits:
Humans, Randomized Controlled Trial,
Meta-Analysis, All Child (0-18 years), yielded
175 citations. A simultaneous Cochrane Library
search for "severe malaria" in ‘Record Title’
listed 4 Cochrane reviews, 7 other systematic
reviews and 98 clinical trials. Three relevant
Cochrane reviews compared quinine with (i)
artesunate(5), (ii) arteether(6) and (iii)
artemisinin derivatives(7). The artesunate review(5)
included one pediatric trial, but examined effects
across all age groups together. The arteether
review(6) examined only the intramuscular route, and
the third review(7) was closed by the authors in
2009 in view of more recent reviews. Six of seven
non-Cochrane reviews compared artesunate or
artemether, but all were outdated. This necessitates
a fresh systematic review to generate current best
evidence.
From the literature search, 45
randomized trials were short-listed, but 42 excluded
for the following reasons: (i) not RCT
comparing artemisinin derivatives vs quinine (n=16),
(ii) adult participants (n=12), (iii)
trials included children also, but presented data
for adults and children together (n=3), (iv)
outdated meta-analysis of trials (n=3), (v)
trials compared different preparations/routes of
Artemisinin without a quinine comparator (n=6), and
(vi) severe malaria not defined as per
standard criteria (n=2). Hand-searching of
short-listed citations identified 7 additional
trials; thus a total of 10 trials were included in
this review.
Table I summarizes the
trial characteristics. Two trials compared quinine
with artesunate(8,9), six with artemether(10-15),
and two with arteether(16,17). Four trials recruited
only participants with cerebral
malaria(10,11,13,14). The trials examined mortality,
clinical outcomes (fever clearance time, coma
recovery time, neurological sequelae), parasite
clearance and some side effects.
Table I
Characteristics of Included Trials
|
Trial |
Setting |
Participants |
Inclusion criteria |
N (A/Q) |
Administration |
Outcomes |
|
Artesunate |
|
Phuong, et al.(8) |
Vietnam |
<15 y |
PS + CF of severe |
37/35 |
A = im# |
Mortality |
| |
year NS |
|
malaria* |
|
Q = iv*** + |
FCT, CRT, |
| |
|
|
|
|
mefloquine po |
PCT, LOS |
|
Mohanty, et al.(9) |
India |
Pediatric, |
PS + CF of severe |
40/40 |
A = iv## |
Mortality, |
| |
2000-02 |
but age NS |
malaria* |
|
Q = iv*** |
FCT,
CRT, PCT, AE, |
|
Artemether |
|
Murphy, et al.(10) |
Kenya |
<12 y |
PS + CF of |
83/78** |
A = im$ |
Mortality, CRT, |
| |
year NS |
|
cerebral malaria |
|
Q = iv*** |
neurological
sequelae |
|
vanHensbroek, et al(11) |
Gambia |
1-9 y |
PS + CF of |
288/288 |
A = im$ |
Mortality, |
| |
1992-94 |
|
cerebral malaria |
|
Q = im*** |
FCT, CRT, PCT, AE |
|
Taylor, et al.(12) |
Malawi |
Pediatric, |
PS + CF of |
95/88 |
A = im$ + |
Mortality, FCT, |
| |
1992-94 |
but
age NS |
severe malaria* |
|
Pyrisulpha |
CRT, PCT, AE, |
| |
|
|
|
|
Q = iv*** |
neurological sequelae |
|
Ojuawo, et al.(13) |
Nigeria |
2-6 y |
PS + CF of |
18/19 |
A = im$ |
Mortality, |
| |
year NS |
|
cerebral malaria |
|
Q = iv*** |
FCT, CRT, PCT, |
| |
|
|
|
|
|
neurological sequelae |
|
Olumese, et al.(14) |
Nigeria |
11mo-5y |
PS + CF of |
54/59 |
A = im$ |
Mortality, |
| |
1994-96 |
|
cerebral malaria |
|
Q = iv*** |
FCT,
CRT, PCT, AE, |
| |
|
|
|
|
|
neurological sequelae |
|
Huda, et al.(15) |
India |
<14 y |
PS + CF of s |
23/23**** |
A = im$$ |
Mortality, |
| |
2000-01 |
|
evere malaria* |
|
Q = iv*** |
FCT, CRT, PCT, |
| |
|
|
|
|
|
neurological sequelae |
|
Arteether |
|
Moyou-Somo, et al.(16) |
Cameroon |
0-10y |
PS + CF of |
51/51 |
A = im$ |
Mortality, |
| |
1995-97 |
|
severe malaria* |
|
Q = iv*** |
FCT, CRT, PCT, |
| |
|
|
|
|
|
neurological sequelae |
|
Thuma, et al.(17) |
Zambia |
0-10y |
PS + CF of |
48/44 |
A = im$ |
Mortality, |
| |
1996-97 |
|
severe malaria* |
|
Q = iv*** |
FCT,
CRT, PCT, |
| |
|
|
|
|
|
neurological sequelae |
A = Artemisinin derivative, AE = adverse events, CF = clinical features, CRT = coma recovery time,
FCT = fever clearance time, im = intramuscular, iv = intravenous, LOS = length of stay in hospital,
N = number of participants, NS = not specified, PCT = parasite clearance time, po = per oral,
PS = peripheral smear showing asexual forms of Plasmodium falciparum, Pyri-sulpha = pyrimethamine-sulphadoxine,
Q = Quinine; *Clinical features consistent with WHO categorisation of severe malaria;
** 200 were enrolled, but 161 analysed; *** Quinine dose 20 mg/kg loading followed by 10mg/kg 8 hourly until
conscious for a total of seven days; **** 99 were enrolled, but 46 analysed;
# Artesunate dose 3mg/kg followed by 2mg/kg at 12, 24, 48, 72 hr + mefloquine orally;
##Artesunate dose 2.4 mg/kg loading followed by 1.2 mg/kg after six hours and once a day for five days;
$Artemether/Arteether dose 3.2 mg/kg followed by 1.6 mg/kg for four days;
$$Artemether dose 1.6 mg/kg bd followed by 1.6 mg/kg od for five days
|
Risk of bias (Table II)
was low for three trials(11,12,14), moderate for
another three(8,10,17) and high for four
trials(9,13,15,16). Only one trial(11) provided a
sample size calculation. None of the trials was
blinded.
Table II
Risk of Bias and Other Design Characteristics of Included Trials (Cochrane Risk of Bias Tool)
|
Trial |
Randomization |
Allocation |
Blinding |
Adequacy |
ITT |
Risk |
Sample size |
Ref |
|
|
|
concealment |
|
of outcome |
analysis |
of |
|
|
|
|
|
|
|
reporting |
|
Bias |
|
|
|
Phuong |
Unclear |
Adequate |
Inadequate |
Adequate |
Yes |
Moderate |
Inadequate |
8 |
|
Mohanty |
Inadequate |
Inadequate |
Inadequate |
Inadequate |
No |
High |
Inadequate |
9 |
|
Murphy |
Adequate |
Adequate |
Inadequate |
Inadequate |
No |
Moderate |
Inadequate |
10 |
|
vanHensbroek |
Adequate |
Adequate |
Inadequate |
Adequate |
Yes |
Low |
Adequate |
11 |
|
Taylor |
Adequate |
Adequate |
Inadequate |
Adequate |
No |
Low |
Inadequate |
12 |
|
Ojuawo |
Inadequate |
Inadequate |
Inadequate |
Adequate |
No |
High |
Inadequate |
13 |
|
Olumese |
Adequate |
Adequate |
Inadequate |
Adequate |
Yes |
Low |
Inadequate |
14 |
|
Huda |
Inadequate |
Inadequate |
Inadequate |
Inadequate |
No |
High |
Inadequate |
15 |
|
Moyou-Somo |
Adequate |
Inadequate |
Inadequate |
Inadequate |
No |
High |
Inadequate |
16 |
|
Thuma |
Adequate |
Adequate |
Inadequate |
Inadequate |
No |
Moderate |
Inadequate |
17 |
|
ITT = intention-to-treat |
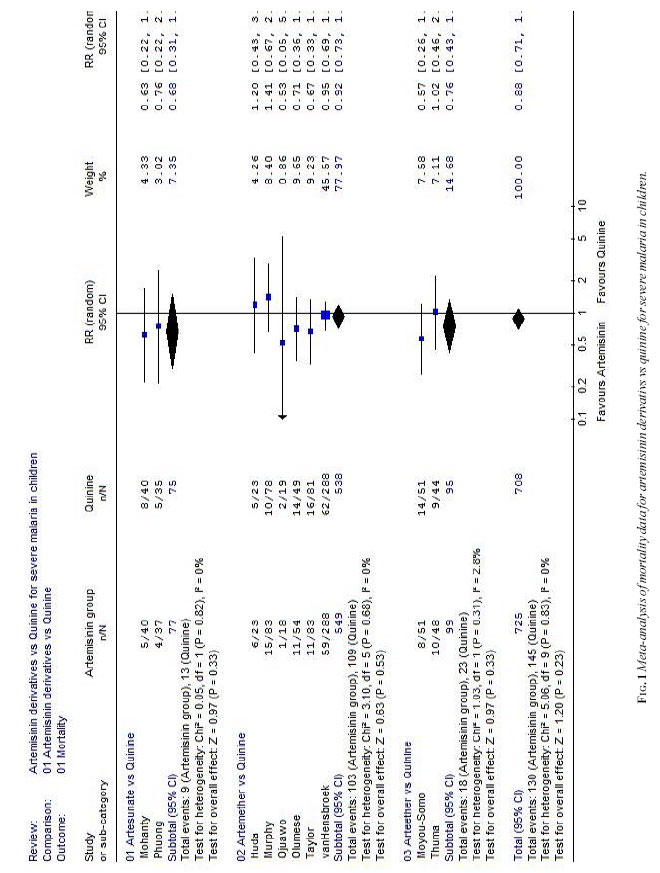
All the ten trials demonstrated
comparable mortality between artemisinin derivatives
and quinine; irrespective of the type of derivative,
route of administration, type of severe malaria
(cerebral or otherwise), or methodological quality
of trial. Meta-analysis(Figure I) confirmed
this for artemisinin derivatives individually and
collectively (both random effects and fixed effect
model). The trials together included a sample size
sufficient for demonstrating a statistically
significant mortality reduction, suggesting that the
result is robust.
Seven trials reported fever
clearance time, though three(8,11,12) presented data
in a format that precluded meta-analysis; the
remainder(9,15-17) showed comparable results between
all three artemisinin derivatives and quinine. All
trials reported coma recovery time, though
three(8,11,12) could not be included in
meta-analysis. Only one trial(13) suggested a
favourable effect with artemether; the remainder
showed no difference between groups. Likewise
parasite clearance time was comparable between
groups in five trials(8,9,11,12,17). Six
trials(10,12-14,16,17) examined neurological
sequelae at follow-up, and all showed comparable
effect between artemisinin and quinine.
Critical Appraisal
This is the first systematic
review examining the scope of artemisinin
derivatives for severe malaria in children. Despite
several methodological strengths (multiple database
search, hand-searching, methodo-logical grading,
standard reporting format, meta-analysis, etc), one
of its limitations was the inability to obtain
separate pediatric data from trials(18-20) combining
adult and pediatric data.
On the face of it, this
systematic review appears to corroborate the WHO
position that there is inadequate evidence favouring
artemisinin derivatives in severe childhood
malaria, suggesting the need for more RCTs(1).
However, this may be an over-simplification, because
although the review does not demonstrate superior
efficacy of artemisinin derivatives, comparable
effect across all outcomes suggests that either
therapy could be equally efficacious. Given that
quinine administration requires controlled infusion
in a hospital setting, artemisinin could have an
edge in terms of simpler administration and
potentially greater safety (lower risk of quinine
adverse events). Since treatment of severe malaria
in the real-world setting is often presumptive
(before confirmation of diagnosis), and urgent
(required before transferring patients to hospital),
unlike in randomized trials, Artemisinin may result
in greater effectiveness, despite equivalent
efficacy. This is especially important because
neither the absence of P.falciparum on
peripheral smear nor the presence of P.vivax,
rule out severe malaria(2).
However, potentially better
‘effectiveness’ has to be counterbalanced against
the possible risk of encouraging Plasmodium
resistance through relatively unrestricted use of
artemisinin derivatives. Thus a dichotomy between
the interests of the individual child and the
community could emerge over time. This suggests that
a formal Health Technology Assessment rather than
the simplistic decision models described
earlier(2-4) is needed to make an informed choice.
Extendibility
All the trials were conducted in
developing countries, although mostly in Africa
where the severity and outcome of malaria could be
different from our country. However, the type of
participants, clinical classification of severity,
outcome parameters and overall results were similar
between the Indian(9,15) and other trials. This
suggests that the findings of this systematic review
can be extended to our country in general.
Funding: None.
Competing interest: None
stated.
|
EURECA Conclusion in the Indian Context
• In children with severe
malaria, Artemisinin derivatives result in
similar mortality and clinical outcomes, as
compared to parenteral quinine.
• Non-inferior efficacy
could permit preferential use of Artemisinin,
owing to simpler administration and
potentially greater safety at the
point-of-care, especially in field settings.
|
References
1. Guidelines for the treatment
of malaria. Second Edition. World Health
Organization, 2010. Available at http://www.rollbackmalaria.org/docs/hbsm.pdf
on 25 March, 2010.
2. Guidelines for diagnosis and
treatment of malaria in India. Government of India,
2009. Available at http://www.mrcindia.org/Guidelines_for
_Diagnosis_Treatment.pdf. Accessed on 25 March,
2010.
3. Kundu R, Ganguly N, Ghosh TK,
Choudhury P, Shah RC. Diagnosis and management of
malaria in children. Recommendations and IAP plan of
action. Indian Pediatr 2005; 42: 1101-1114.
4. Infectious Diseases Chapter,
Indian Academy of Pediatrics. Management of malaria
in children: Update 2008. Indian Pediatr 2008; 45:
731-735.
5. Jones KL, Donegan S, Lalloo
DG. Artesunate versus quinine for treating severe
malaria. Cochrane Database Syst Rev 2007; 4:
CD005967.
6. Afolabi BB, Okoromah CAN.
Intramuscular arteether for treating severe malaria.
Cochrane Database Syst Rev 2004; 4: CD004391.
7. McIntosh H, Olliaro P.
Artemisinin derivatives for treating severe malaria.
Cochrane Database Syst Rev 2000; 2: CD000527.
8. Phuong CXT, Bethell DB, Phuong
PT, Mai TTT, Thuy TTN, Ha NTT, et al.
Comparison of artemisinin suppositories,
intramuscular artesunate and intravenous quinine for
the treatment of severe childhood malaria. Trans R
Soc Trop Med Hyg 1997; 91: 335-342.
9. Mohanty AK, Rath BK, Mohanty
R, Samal AK, Mishra K. Randomized control trial of
quinine and artesunate in complicated malaria.
Indian J Pediatr 2004; 71: 291-295.
10. Murphy S, English M, Waruriu
C, Mwangi I, Amoukoye E, Crawley J, et al. An
open randomised trial of artemether versus quinine
in the treatment of cerebral malaria in African
children. Trans R Soc Trop Med Hyg 1996; 90:
298-301.
11. van Hensbroek MB, Onyiorah E,
Jaffar S. A trial of artemether or quinine in
children with cerebral malaria. N Engl JMed 1996;
335: 69-75.
12. Taylor TE, Wills BA, Courval
JM, Molyneux ME. Intramuscular artemether vs
intravenous quinine: An open, randomized trial in
Malawian children with cerebral malaria. Trop Med
Int Health 1998; 3: 3–8.
13. Ojuawo A, Adegboye AR,
Oyewalw O. Clinical response and parasite clearance
in childhood cerebral malaria: A comparison between
intramuscular artemether and intravenous quinine.
East Afr Med J 1998; 75: 450-452.
14. Olumese PE, Bjorkman A,
Gbadegesin RA, Adeyemo AA, Walker O. Comparative
efficacy of intramuscular artemether and intravenous
quinine in Nigerian children with cerebral malaria.
Acta Tropica 1999; 73: 231-236.
15. Huda SN, Shahab T, Ali SM,
Afzal K, Khan HM. A comparative clinical trial of
artemether and quinine in children with severe
malaria. Indian Pediatr 2003; 40: 939-945.
16. Moyou-Somo R, Tietche F,
Ondoa M, Kouemeni LE, Ekoe T, Mbonda E, et al.
Clinical trial of beta-arteether versus quinine
for the treatment of cerebral malaria in children in
Yaounde, Cameroon. Am J Trop Med Hyg 2001; 64:
229-232.
17. Thuma PE, Bhat GJ, Mabeza GF,
Osborne C, Biemba G, Shakankale GM, et al. A
randomized controlled trial of artemotil (beta-arteether)
in Zambian children with cerebral malaria. Am J Trop
Med Hyg 2000; 62: 524-529.
18. Dondorp A, Nosten F,
Stepniewska K, Day N, White N; South East Asian
Quinine Artesunate Malaria Trial (SEAQUAMAT) group.
Artesunate versus quinine for treatment of severe
falciparum malaria: a randomised trial. Lancet 2005;
366: 717-725.
19. Esamai F, Ayuo P, Owino-Ongor
W, Rotich J, Ngindu A, Obala A, et al. Rectal
dihydroartemisinin versus intravenous quinine in the
treatment of severe malaria: a randomised clinical
trial. East Afr Med J 2000; 77: 273-278.
20. Fargier JJ, Louis FJ, Duparc
S, Hounsinou C, Ringwald P, Danis M. Comparative
study of artemether and quinine in severe Plasmodium
falciparum malaria in adults and older children in
Cameroon. Med Trop (Mars) 1999; 59: 151-1516.
|
|
|
 |
|