|
|
|
Indian Pediatr 2009;46: 383-388 |
 |
Comparison of Ready-to-Use Therapeutic Food
with Cereal Legume-based Khichri Among Malnourished
Children |
|
Brinda Dube, Temsunaro Rongsen, Sarmila Mazumder, Sunita Taneja, Farhana
Rafiqui,
Nita Bhandari and M K Bhan
*
From the Society for Essential Health Action and
Training, New Delhi, India; and *Department of Biotechnology, Ministry of
Science and Technology, Government of India, New Delhi, India.
Correspondence to: Dr Nita Bhandari, Society for
Essential Health Action and Training, B-10 Soami Nagar, New Delhi 110 017,
India. E-mail:
[email protected]
Manuscript received: November 28, 2007; Initial Review
completed: March 10, 2008;
Accepted: June 20, 2008.
|
|
Abstract
Objective:
To compare the acceptability and energy intake of Ready-to-Use
Therapeutic Food (RUTF) with cereal legume based khichri among
malnourished children.
Design: An acceptability trial with cross-over
design.
Setting: Urban low to middle socioeconomic
neighbor-hoods in Delhi.
Subjects: 31 children aged
³6 to £36 months with malnutrition,
defined as Weight for height (WHZ) <–2 to ³–3 SD, with no clinical signs
of infection or edema.
Intervention: Children were offered weighed
amounts of RUTF and khichri in unlimited amounts for 2 days, one
meal of each on both days. Water was fed on demand. Caregivers’
interviews and observations were conducted on the second day.
Outcome Measures: Acceptability of RUTF compared
to khichri based on direct observation and energy intake for test
and control meals.
Results: The proportion of children who accepted
RUTF eagerly was 58% as against 77% for khichri. 42% children on
RUTF and 23% on khichri accepted the meal but not eagerly. The
median (IQR) energy intake over the two day period in children aged 6 to
36 months from RUTF was 305 (153, 534) kcal, and from khichri was
242 (150, 320) kcal (P=0.02).
Conclusion: RUTF and khichri were both
well accepted by study children. The energy intake from RUTF was higher
due to its extra energy density.
Keywords: Acceptability, Khichri, Malnourished, Ready-to-use
therapeutic food (RUTF).
|
|
WHO recommends that severely malnourished children be fed for a few days
on a low protein, low energy diet (F75) containing 75 kcal and 0.9 g
protein/100 mL, fortified with vitamins and minerals, until life
threatening complications are in control(1). The rehabilitation phase then
begins with an energy and protein dense (100 kcal and 2.9 gm protein/100
mL) milk based diet (F100) fortified with a vitamin mineral (CMV) mix to
promote rapid weight gain. The F100 diet is not recommended for use at
home as it requires water for reconstitution, which facilitates growth of
pathogenic bacteria. The risk of bacterial contamination with F100 is
therefore high, and it needs to be prepared before each meal and cannot be
prepared and stored for multiple feeds. Further, F100 resembles infant
formula and its promotion may negatively impact breastfeeding. WHO has
recommended development of an alternate therapeutic diet which can be used
at the community level(1).
In India, khichri (rice and green gram gruel) is
often used for the dietary management of moderately malnourished children
as a practical and culturally acceptable food for young children. However,
khichri is required to be fed several times and this is difficult
for caregivers because the recipe requires cooking and reheating before it
is offered each time. Besides, green gram is costly for poor communities,
where most malnourished children reside. Also, khichri is a good
medium for bacterial growth.
An alternative solid ready-to-use therapeutic food (RUTF)
has been developed(2-4). RUTF has a 5 times greater energy density than
F100 but a similar nutrient to energy ratio. Part of the dried skim milk
in F100 is replaced with a mixture of peanut butter and lacto serum, and
oil by vegetable fat mixture, including essential fatty acids with
adequate viscosity and melting point to produce the RUTF(2,3). RUTF has a
high concentration of micronutrients and vitamins whose unpleasant taste
is well masked(2-4). The child can consume RUTF without adding water,
unlike the F100. Thus, the risk of bacterial growth and proliferation is
reduced. These characteristics make RUTF a safer intervention in
communities. Besides, RUTF does not require cooking.
In Africa, RUTF has shown excellent acceptability in
cross over or comparative trials(2,3). The acceptability of this new high
energy dense food is important to assess in India before its practical use
can be addressed in the country. We conducted a preliminary study to test
the acceptability and energy intake of RUTF as compared to commonly used
cereal legume gruel (khichri). We anticipate that the study
findings would provide a basis for planning large scale evaluations of
RUTF.
Methods
The setting was the urban low to middle socioeconomic
neighborhoods of Tigri in South Delhi. The population characteristics have
been described elsewhere(5,6). Childhood malnutrition is common in this
setting(7,8). The study was approved by the ethics committee of the
Society for Applied Studies.
Sample size: Two studies comparing the intake from
RUTF and F100 showed that the difference in intake to be expected between
the two feeds was about 1 SD(2,4). To obtain a difference significant at
the 0.05 percent level with 95% power, a minimum of 26 children were
needed. To allow for dropouts and missing data, we planned enrolment of 30
children. Forty children were identified to account for dropouts during
the ‘pretesting’ phase, due to illness and refusals.
Enrolment: A door to door survey was conducted, to
identify children aged 6 to 36 months. Subsequent to obtaining consent,
the child’s weight (Seca scale with sensitivity 25g) and length (infantometer
with sensitivity of 0.1 cm) were taken by three anthropometrists. These
three anthropometrists underwent several sessions of intra and inter
observer standardization exercises. Exercises were conducted till there
was no difference in weight measurements and only a ±0.2cm in length
measurements among the three. Consent for participation was taken from
families of children whose weight for height was <–2 to
³–3SD
according to the WHO growth standards(9), and clinically free of signs of
infection and edema(10).
The acceptability trial involved feeding of two meals a
day, one of each type (RUTF and khichri) for two days. Prior to
initiating the trial, the 36 potentially eligible children underwent a
‘pretesting’ phase. During this pretesting phase, khichri and RUTF
were given for two days to the caregiver to be fed at 2 meals each (one
meal of each on both days) to familiarize the mother and child with the
diet.
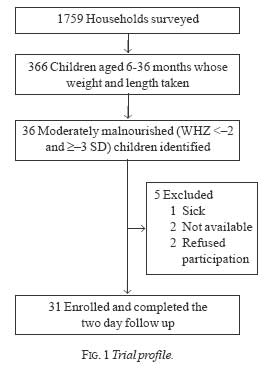
Of the 36 children who participated in the pre-testing,
31 children were enrolled in the main trial (Fig.1). The
trial children were brought to the study clinic set up in Tigri on two
consecutive days. The 31 children when assessed using the Integrated
Management of Neonatal and Childhood Illness protocol(11) did not reveal
presence of local or systemic bacterial infection. After obtaining consent
again, they were enrolled into the study.
Randomization: The study had a cross over
design. The randomization list for the sequence in which meals would be
fed to a particular child on the two days was generated offsite by a
statistician not otherwise involved with the study. Using a simple
randomization scheme, half the participants were assigned to receive
khichri and the other half RUTF as their first meal on the first day.
The other food i.e. khichri or RUTF was given as the second meal on
the first day. The food received by a child at the second meal on the
first day was administered as the first meal on the second day (i.e.
if khichri was the second meal on day 1, khichri was given
as first meal on the second day of the observation). Each enrolled child
received four meals; one meal of khichri and one of RUTF on each of
the two days.
Intervention: The energy and nutrient
content of the two foods i.e. RUTF and khichri is given in
Table I. Khichri was prepared using rice (100 g),
green gram (60 g), groundnut oil (20 mL), spinach (100 g) and water (640
mL). 760 g of khichri so prepared yielded 760 kcal i.e. 1 kcal/g of
cooked khichri (Table I). The energy content for
khichri was calculated using national food composition tables(12).
TABLE I
Nutritive Value of RUTF and Khichri per 100 Grams
| Nutrients |
RUTF |
Khichri |
| Energy (kcal) |
545 |
100 |
| Proteins (g) |
13.6 |
3.1 |
| Lipids (g) |
35.7 |
2.9 |
| Minerals |
|
Calcium (mg) |
320 |
16.8 |
|
Phosphorus (mg) |
394 |
55.8 |
|
Potassium (mg) |
1111 |
117.9 |
|
Magnesium (mg) |
92 |
29.9 |
|
Sodium (mg) |
189 |
9.8 |
|
Iron (mg) |
11.5 |
0.5 |
|
Zinc (mg) |
14 |
0.4 |
|
Copper (mg) |
1.78 |
0.06 |
|
Iodine (µg) |
110 |
|
|
Selenium (µg) |
3 |
|
| Vitamins |
|
Vitamin A (mg) |
0.91 |
0.20 |
|
Vitamin D (µg) |
16 |
|
|
Vitamin E (mg) |
20 |
|
|
Vitamin C (mg) |
53 |
3.7 |
|
Vitamin B1 (mg) |
0.6 |
0.05 |
|
Vitamin B2 (mg) |
1.8 |
0.06 |
|
Vitamin B6 (mg) |
0.6 |
|
|
Vitamin B12 (µg) |
0.53 |
|
|
Vitamin K (µg) |
21 |
|
|
Folic acid (µg) |
210 |
28.3 |
|
Ca D Pantothenate (mg) |
3.1 |
|
|
Biotin (µg) |
65 |
|
|
Niacin (mg) |
5.3 |
0.5 |
Children were offered the food that they were scheduled
at two meals at 10 am and 2 pm on each of the two days. The meal time
lasted an hour. Caregivers were instructed to feed their children and to
encourage them to eat as much as they could of the pre-weighed food in the
one hour period. If children ate the preweighed amount, the initial amount
was reoffered. Measured volumes of plain water was also given in between
the meals. Caregivers were asked not to feed the child any other foods
during the interval between the two feeds. Once the meal time was over,
the foods were weighed again and the amount of food consumed in grams was
estimated. The leftover water was also measured to estimate the volume of
water consumed.
Prior to commencing meals on the second day, each child
was again examined for local and systemic infections and none of the
children had either of these.
Observation of feeds and interviews with caregivers:
Observations were conducted on each child on the second day for both
the meals. An observation checklist was used to observe the child for a
minute after every 15 minutes i.e. a total of 4 observations per child
were obtained for khichri and RUTF. Caregivers of all enrolled
children were also interviewed by nutritionists using a semi-structured
questionnaire to enquire about their perceptions about the RUTF.
Analysis: Acceptability was categorized as
‘accepted eagerly’ if they ate food readily, did not make a fuss, spit
out, vomit or cry during the observed meal. Children were categorized as
‘accepted but not eagerly’ if they ate the offered food but either made
fuss, spit out, vomited or cried during the observed meal. The third
category was children who did not consume the offered food at all.
A summary variable was created from the 4 observations
for each food observed i.e. RUTF and khichri. The higher
category of acceptability was assigned if the defined behavior was
observed in at least two observations. The categories of acceptability
across RUTF and khichri were compared by Pearson chi-square test.
Energy intakes were estimated from the amount (in
grams) of each food consumed by a child at each meal. The difference in
median energy intakes for both foods on the two days was estimated between
the two groups and compared by a Wilcoxon signed rank test.
Results
Among the 31 trial subjects, 16 (51.6%) were male.
Eight, 19 and 4 children were aged 6 to 12, 13 to 24 and 25 to 36 months,
respectively. Table II depicts the acceptability of RUTF and
khichri. Table III provides the amount of RUTF and
khichri consumed and the energy intakes in the two groups.
TABLE II
Acceptability of RUTF and Khichri
|
Acceptability |
RUTF |
Khichri |
P |
|
|
n = 31 |
n = 31 |
value* |
|
Accepted eagerly |
18 |
24 |
0.35 |
|
Accepted, but not eagerly |
13 |
7 |
0.35 |
|
*Chi square test |
TABLE III
Intake of RUTF and Khichri From Two Meals Offered in Unrestricted Amount on Two Consecutive Days
| |
n |
RUTF |
Khichri |
P value* |
| Amount
consumed (g) |
31 |
56 (28, 98) |
242 (150, 320) |
<0.0001 |
| Energy
intake (Kcal) |
31 |
305.2 (153, 534) |
242 (150, 320) |
0.02 |
| Children
aged 6-11 months |
8 |
234.3 (185.3,327) |
149 (107, 204) |
0.01 |
| Children
aged 12-36 months |
23 |
316.1 (141.7,545) |
290 (178, 374) |
0.11 |
|
All values are median (IQR); *Wilcoxon signed rank test |
During the interviews with caregivers, 22 (71%) of the
31 caregivers reported that their children had liked the RUTF. The common
reasons stated for liking RUTF were that children ate most of the portion
served to them (22/22), child asked for more (3/22), did not make a fuss
about eating (2/22), smacked his lips (1/22), never used to eat any food
but ate RUTF (1/22) and that the child started passing a single stool per
day (1/22). Nine (29%) caregivers reported that RUTF was not liked by
their children; the most common reasons were children did not eat enough
of the food (8/9), grimaced while being fed (1/9), spat out the food (1/9)
and refused to eat it (3/9).
Twenty eight of the 31 caregivers thought the
consistency of RUTF was appropriate for children, the appearance (packet
and color) was good (10/28), the food looked like chocolate (3/28), their
child ate it (1/28) and it gave more energy than home foods (2/28). Three
caregivers felt the consistency was thick and therefore inappropriate for
children. However, two of them had reported that their children had liked
the food when asked so. Caregivers were also asked whether they would feed
RUTF to their children if it were available to them in the future. Of the
31 interviewed, 29 said that they would use it; the reasons cited were
that it gave energy to their children (22/29), their children liked it
(11/29) and it increased the child’s appetite (3/29). Less common reasons
were that it will protect the child from disease (1/29), the child’s
weight will increase (1/29), it is like chocolate (1/29), it will improve
child’s health (1/29) and that the government always gives products that
are beneficial for children (1/29). Only 2 (6.4%) caregivers said they
would not give it because their children did not like it (1/2) or eat it
(1/2).
Discussion
In this preliminary trial, while both khichri
and RUTF were accepted well by young children, acceptability of khichri
was somewhat better. Khichri is a culturally acceptable and
palatable meal and widely consumed by families and children in this
setting. Under conditions of unlimited access at each of the test meals,
the intake of RUTF was lower but the energy intake from it was
significantly higher. The energy density for RUTF was five fold higher and
this would explain the lower consumption as well as the substantially
higher energy intake.
The findings of this study are consistent with previous
reports; improved energy intakes were reported in severely malnourished
children in two other studies that compared RUTF with the F100 diet(2,4).
In a therapeutic feeding centre in, Chad, in severely malnourished
children, Briend, et al.(2) observed a two fold higher mean energy
intake from RUTF as compared to F100 diet. In another study from Senegal,
also in severely malnourished children, the mean daily energy intake was
70% higher in the RUTF group(4).
An important question to address is whether a product
like RUTF has a potential use under special circumstances and whether a
more decisive safety or efficacy evaluation is merited. RUTF has been
proposed as potentially useful in situations of war and disaster, in home
treatment of severe malnutrition when hospitalization is not feasible or
in centres without a kitchen, or as an add-on in health facilities where
diets can only be offered 2 or 3 times a day. This would require
assessment of its use in less supervised circumstances. Further RUTF has
been less well studied in infants and in malnourished children with
infections. Clearly RUTF does not have a role in settings where standard
treatment of malnutrition is feasible. As it avoids problems of quality
control and microbial contamination, RUTF may be considered for evaluation
in difficult circumstances where standard protocols are not feasible to
implement.
Acknowledgment
We are grateful to Dr Andre Briend for his constructive
inputs and for reviewing the manuscript. We thank Ms Baljeet Kaur for help
in statistical analysis.
Contributors: BD, TR, NB and MKB were
involved in concept and protocol design, oversight of all phases of the
trial, and interpretation, preparation and finalization of manuscript. SM,
ST and FR were involved in the review of literature, analysis and
interpretation of manuscript. BD and FR collected the data under
supervision of TR and NB.
Funding: World Health Organization, Geneva.
Competing Interests: None stated.
|
What is Already Known?
• RUTF (Ready to Use Therapeutic Food) is a
nutrient dense spread with a nutritional value close to WHO F100 and
has been developed for the treatment of severely malnourished
children.
What This Study Adds?
• RUTF is well accepted and provides higher energy intakes than
equivalent number of meals of khichri. |
References
1. World Health Organization. Management of severe
malnutrition: a manual for physicians and other senior health workers.
Geneva, Switzerland: World Health Organization; 1999.
2. Briend A, Lacsala R, Prudhon C, Mounier B, Grellety
Y, Golden MH. Ready-to-use therapeutic food for treatment of marasmus.
Lancet 1999; 353: 1767-1768.
3. Briend A. Highly nutrient-dense spreads: a new
approach to delivering multiple micronutrients to high-risk groups. Br J
Nutr 2001; 85 Suppl 2: S175-S179.
4. Diop EHI, Dossou NI, Ndour MM, Briend A, Wade S.
Comparison of the efficacy of a solid ready-to-use food and a liquid,
milk-based diet for the rehabilitation of severely malnourished children:
a randomized trial. Am J Clin Nutr 2003; 78: 302-307.
5. Bhandari N, Bahl R, Taneja S, Strand T, Molbak K,
Ulvik RJ, et al. Substantial reduction in severe diarrheal
morbidity by daily zinc supplementation in young north Indian children.
Pediatrics 2002; 109: 86-92.
6. Bhandari N, Bahl R, Taneja S, Strand T, Molbak K,
Ulvik RJ, et al. Effect of routine zinc supplementation on
pneumonia in children aged 6 months to 3 years: randomized controlled
trial in an urban slum. Br Med J 2002; 324: 1358-1362.
7. Bhandari N, Bhan MK, Sazawal S. Impact of massive
dose of vitamin A given to preschool children with acute diarrhea on
subsequent respiratory and diarrheal morbidity. Br Med J 1994; 309:
1404-1407.
8. Bhandari N, Bahl R, Hambidge KM, Bhan MK. Increased
diarrheal and respiratory morbidity in association with zinc deficiency -
a preliminary report. Acta Pediatr 1996; 85: 148-150.
9. World Health Organization. The WHO Child Growth
Standards. Available from http://www.who.int/childgrowth/standards/en/.
Accessed May 26, 2008.
10. World Health Organization. Integrated Management of
Childhood Illness (WHO/CHD/97.3E). Geneva, Switzerland: World Health
Organization; 1997.
11. Government of India. Integrated Management of
Neonatal and Childhood Illnesses: Health Worker Chart Booklet. New Delhi,
India: Ministry of Health and Family Welfare; 2003: 5-6.
12. Gopalan C, Sastri BVR, Balasubramanian SC, Rao N,
Deosthale YG, Pant KC. Nutritive value of Indian Foods. Hydrabad, India:
National Institute of Nutrition, Indian Council of Medical Research; 1999.
|
|
|
 |
|