|
|
Case Reports Indian Pediatrics 2008;45:415-417 |
||||||
|
Septic Pulmonary Embolism in a Child |
||||||
|
Solmaz Celebi
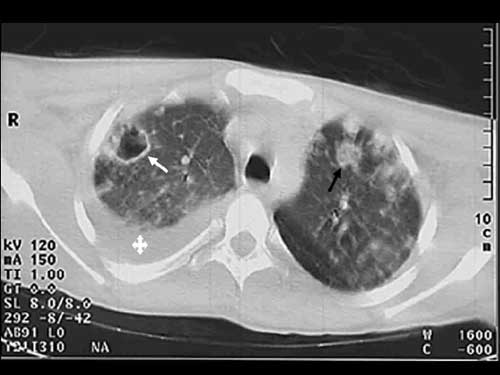
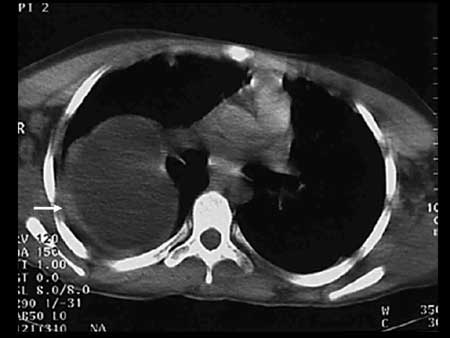
: Children, Septic pulmonary embolism, Staphylococcus aureus. Introduction Septic pulmonary embolism (PE) is an uncommon condition in children(1). Numerous pulmonary infarcts resulting from small emboli may be associated with right sided bacterial endocarditis, septic thrombophlebitis and osteomyelitis(2). The clinical picture is variable, often suggests pneumonia and the diagnosis may not be established until autopsy(3). Septic PE usually presents as fever, hemoptysis and patchy infiltrates on chest radio-graphs(4). We hereby present a case of septic PE in a child. Case Report A previously healthy 15-year-old girl with a 5-day history of sprain in the right ankle was admitted to emergency ward. She presented with fever, pain, erythema, and swelling on the left leg, left arm and right ankle. Physical examination showed fever of 38.5ºC; wide-spread rales on right lung fields, swelling, erythema and tenderness at the left leg, left arm and right ankle. Laboratory analysis showed white blood cell count of 7800/mm³ (72% neutrophils, 22% lymphocytes, 4% monocytes, 2% eosinophils), hemoglobin 12.4 g/dL, platelet 172000/mm³, erythrocyte sedimentation rate 30 mm/h and C-reactive protein 7.5 mg/dL. Chest radiograph revealed large sized round density in the right lung and consolidation areas in peripheral portions of both lungs (Fig 1). There was soft tissue swelling on extremity radiographs. At the begining cefotaxime and clindamycin were initiated for soft tissue infection, however clindamycin was later replaced with vancomycin, because of suspicion of methicillin resistant Staphylococcus aureus (MRSA) infection. By the second hour, she had developed progressive respiratory distress and fever. Computed tomography (CT) showed bilateral multiple round and cavitary nodules in peripheral portions of both lungs and, pleural effusion in the right lung (Fig 2). Other chest CT section revealed a thin walled, hypodense round lesion (8×4 cm) in the right lower lobe superior segment (Fig 3). Albendazole therapy was also added because we could not rule out the possibility of hydatid cysts. By the 3rd hour of admission, progressive deterioration resulted in respiratory failure, requiring mechanical ventilation. The patient developed septic shock. Septic shock treatment was administered according to our clinic protocol (intravenous fluid, dopamin and adrenalin perfusion). Echocardiography proved normal. By the 5th hour, the patient passed away. Methicillin sensitive Staphylococcus aureus (MSSA) was isolated from blood, pleural fluid and tracheal aspirate fluid cultures. Serum Echinococcus granulosis IgE and its indirect hemagglutination were both negative. Lymphocyte subsets, immuno-globulin level, and tetanus antibody response were normal.
Discussion Septic PE is an uncommon disorder with an insidious onset and is difficult to diagnose(5). Septic PE can progress to abscesses, empyema and bronchopleural fistula(6). Our patient presented with fever as well as signs and symptoms of soft tissue infections. To rule out the possibility of lung abscesses, patient underwent a CT, which showed bilateral multiple round and cavitary nodules in peripheral portions of both lungs and a hypodense lesion (8×4 cm) in the right lower lobe superior segment. Septic PE diagnosis was confirmed by CT in our patient. Typical radiographic features of septic PE include patchy air space lesions simulating nonspecific bronchopneumonia; multiple round or wedge shaped densities of varying sizes from 0.5 to 3.5 cm located peripherally on chest CT scans (7,8). It has been reported that empyema, bronchopleural fistula, pneumothorax, cavity and abscess formations are common in septic PE(7-9). While most frequent underlying cause is a medical device, soft tissue infections may also constitute a focus for septic PE. Wong, et al.(10) reported that the commonest causes of septic PE were soft tissue and bone infections. Primary staphylococcal pneumonia is usually unilateral. In our patient, pulmonary features, include bilateral, peripherally located multiple round and cavitary nodules, rapid progression of cavities and empyema, are compatible with septic embolisation. The cause of septic PE in our patient was staphylococcal bacteremia secondary to soft tissue infection. Staphylococci are the most commonly isolated pathogens in patients developing septic PE(5,10), Anticoagulation is not used in cases of septic embolisation because of higher chances of bleeding in the area of infected embolus and lack of benefit of anticoagulation therapy(6). Eradication of infection is the cornerstone in the management of septic PE(6). Septic embolisation caused by MRSA is best treated with a lactam antibiotic. Our patient was treated with intravenous vancomycin plus cefotaxime, however, she failed to respond to antibiotic therapy. Lee, et al.(11) reported that radiological or surgical interventions were performed on the sites where the emboli originated in addition to antimicrobial therapy. In that study, six patients underwent drainage of the extrapulmonary infection site. Pigtail catheter drainage was performed for liver abscess and for thigh cellulitis(11). In our patient, drainage of the soft tissue infection was not performed due to the rapid deterioration of patient’s condition. Contributors: SC and MH: had primary responsibility for protocol development, and writing the manuscript. MD: contributed to the writing of the manuscript. Funding: None. Competing interest: None stated.
| ||||||
|
References | ||||||
|
![]()