|
|
Case Reports Indian Pediatrics 2001; 38: 546-549 |
||||||
|
Tuberculosis of Lower Cervical Spine |
||||||
|
Tuberculosis of the spine is by far the commonest and certainly the most serious form of osteoarticular tuberculosis(1-4). The disease commonly affects the thoracolumbar spine and infection of the cervical spine is a rare occurrence(5,6). The incidence of involvement of cervial spine is 3%-9.4%(1,2,4,6). Tubercular infection causes destruction, caseation and necrosis of vertebrae, pus forms and may come out of the vertebrae or may present as abscess. The abscess may remain close to the vertebrae and presents on the radiograph as paravertebral or prevertebral abscess or it may move distantly along with tissue planes or along the nerves and vessels to present as cold abscess. The frequency of abscess detection clinically or radiologically varies with the site of the disease, being lowest in the cervical region. Due to relative rarity of the involvement of cervical spine in tuberculosis and further, the frequency of abscess formation being least in the cervical region, we communicate this case.
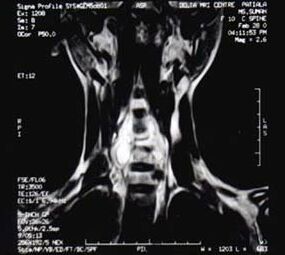
A 10-year-old female child was admitted with history of fever and pain in the neck region for the last 15 days. There was history of vertigo, which increased on standing and walking. The patient complained of generalized body aches and weakness of right hand for the last 7 days. There was no history of trauma in head or neck region. There was no history of headache, vomiting, cough, photophobia, nasal regurgitation, change in voice or any pyogenic focus. No family history of tuberculosis could be traced. On examination, the weight was 27.5 kg. The patient was conscious and afebrile. Pallor was present. Pulse rate was 86 per minute, blood pressure 104/70 mm of Hg. There was no significant lymphadenopathy. Cardio-vascular, respiratory and abdomen examina-tion were normal. Neck rigidity was present. Brudzinski and Kernig’s sign were negative. There was no sign of raised intracranial tension or any cranial nerve involvement. All the deep tendon reflexes were normally elicitable. Movements of right wrist joint were limited and patient was unable to flex at wrist joint and metacarpophalangeal joints. Power was grade 2/6 at the right wrist joint. Local examination of neck showed no deformity, swelling or tenderness. Flexion movements of neck were painful while extension and lateral movements were painless. Investigations revealed hemoglobin of 8 g/dl with total leukocyte count 11,800 per cu mm with 79% neutrophils, 18% lymphocytes, 1% monocytes, 1% basophils and 1% eosinophils. Peripheral blood film showed normocytic hypochromic red blood cells with moderate degree of anisocytosis and poikilocytosis. Sedimentation rate was 25 mm in 1st hour by Westergren method. Cerebrospinal fluid (CSF) examination showed proteins 700 mg, globulins ++++, chlorides 110 meq, and sugar 40 mg/dl as against random blood sugar of 75 mg/dl. Microscopic examination of CSF showed 5 lymphocytes per cu mm. CSF-CRP was negative. Mantoux test was negative and chest X-ray was normal. X-ray of cervical spine showed collapse with destruction of C5 vertebrae, with increased prevertebral soft tissue space. MRI showed caries cervical spine, destruction of C5 vertebral body and intraspinal extension opposite C5 and C6 vertebrae causing compression of thecal sac and spinal cord (Fig. 1). There was large pre and paravertebral mass extending from C3 to C7 which displayed heterogeneous bright signal intensity indicating presence of pus and granulation tissue (Fig. 2). The patient was given antitubercular drugs (rifampicin, isoniazid, pyrazinamide and ethambutol) along with prednisolone for cervical spine tuberculosis and associated tubercular meningitis. Cervical spine was immobilized with cervical collar. The child improved within three weeks of therapy.
Although incidence of tuberculosis of spine in cases of skeletal tuberculosis is quite high, it is a rare occurrence in cervical spine, i.e. 3%-9.4% out of all cases of spinal tuber-culosis(1-4). Involvement of lower cervical spine is a rarity especially below the level of C4(5). Our patient had involvement of 5th cervical vertebrae. The patient also had associated tubercular meningitis as CSF examination revealed raised proteins and globulins while CSF sugar was normal and CSF-CRP was negative. The disease can occur at any age but it is supposed to be a disease of childhood, the maximum occurrence being in the first decade of life(4). Tuli reported that 29% patients of spinal tuberculosis were below 10 years of age and 12% of those had cervical region involvement(7). Among childhood cases, a history of contact is present in about 20% of cases. Common presenting features are back pain, deformity and paraplegia: pain being the commonest in about 75% of the cases. In an early report, 24% patients of cervical spine tuberculosis presented with varying degree of neurological deficit(7). Our patient also presented with fever, pain in neck along with weakness of right hand. The number of the vertebrae involved varies from single vertebra to 14 vertebral segments, average being 3.8 vertebral segments(1). Children seem to have a more severe type of disease than the adults and involvement of more than two vertebrae is frequent in children. In majority of the cases, patients are seen when disease is already well advanced with destruction, collapse and abscess formation. The incidence of abscess formation detected clinically or radiologically is dependent upon the site of disease, lowest being in the cervical region(1,2). MRI is now considered to be the imaging investigation of choice(9). In the present case also MRI showed destruction of vertebral body of C5 and a large pre and paravertebral mass extending from C3 to C7 causing severe cord compression of thecal sac and spinal cord, leading to weakness of right hand. The patients of spinal tuberculosis can be treated non-surgically with four antitubercular drugs, steroids and immobilization(6,8). Our patient also improved with the same therapy. In spinal tuberculosis without neurological signs, immobilization is not always necessary except when cervical spine is involved(9). Decompression of the spinal cord is performed in those cases who don’t show progressive recovery after a fair trial of conservative treatment or in those in whom neurological complication develops during conservative treatment. Treatment by anterior radical excision and interbody bone grafting in patients with spinal tuberculosis and neurological deficit has shown good results(10).
The authors would like to thank Dr. Ravinder Pal Kaur, for help in interpreting the Radiological investigations. Contributors: KKL and MS worked up the case and reviewed the literature. RG and MS drafted the manuscript. KKL will act as the guarantor for the paper. Funding: None. Competing interests: None stated.
|
![]()