|
|
Brief Reports Indian Pediatrics 2001; 38: 534-539 |
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
Evaluation of Growth Hormone Secretion and Insulin-like Growth Factor I in Children with Thalassemia |
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
Growth retardation has been reported to occur in most patients with thalassemia major(1-4). This is believed to be due, at least in part, to a direct effect of iron overload on the endocrine mechanisms of puberty. Growth Hormone (GH) impairment at different levels (hypothalamic or pituitary) and/or reduced insulin like growth factor 1 (IGF-1) synthesis have been suggested to be the main causes of stunned growth in these patients. We, therefore evaluated the relationship between GH, IGF-I and growth parameters in beta-thalassemia patients.
Twenty children with beta-thalassemia major (12 girls and 8 boys), ranging in age from 2 months to 14 years were studied. Height and weight were measured and stand-ard deviation scores (SDS) were calculated according to local standards(5). Bone ages were assessed from hand X-rays according to the Greulich and Pyle Atlas(6). GH stimulation test with oral L-dopa (patients over 22.5 kg, 500 mg; 11 to 22.5 kg., 250 mg; below 11 kg, 125 mg) was performed in every subject and a second test, insulin induced hypoglycemia (ITT: regular insulin, 0.1 U/kg IV) was performed in the subjects whose GH values were below 10 µg/L. GH was measured by RIA (ICN Biomedicals Diagnostics Division, Inc. RSL 124 I Growth Hormone, U.S.). IGF-I was measured in morning serum samples after acid ethanol extraction by RIA (Fa. Nichols, Cal., USA). Reference for normal standards was used from literature(7). IGF-I SDS values were calculated using the formula (IGF-I–1 - mean IGF-I–1)/SD–1 for prepubertal patients and the correction formula (b ´ age + a) was used instead of IGF-I–1 for pubertal children(7). Results were expressed as mean ±SEM and correlation analysis was used as statistical method.
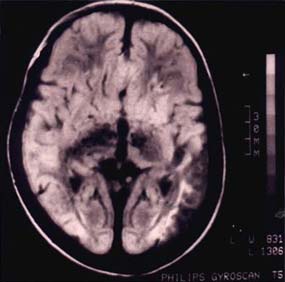
The physical characteristics and the laboratory data of the patients are shown in Tables I and II. The bone age was signi- ficantly lower than the chronological age (p <0.01). We found no significant correlation between height SDS and mean pretransfusion Hb (r = –0.34, p >0.05) or height SDS and mean ferritin levels (r = 0.32, p >0.25). All patients but two responded to L-dopa stimulation test with normal or high GH peaks. ITT stimulation of two nonresponders (Pts No. 17 and 18) also resulted in subnormal GH values (Table II). We found no correlation between ferritin levels and peak GH responses (r = –0.06, p >0.25), but height SDS was strongly correlated with peak GH (r = 0.59, p <0.01). IGF-I levels of the patients were generally below mean of age and sex matched normal children(7). There was no correlation between IGF-I and ferritin (r = 0.08, p >0.25), IGF-I and duration of chelation therapy (r = 0.21, p >0.05) or IGF-I and height SDS (r = 0.22, p >0.05). We found a weak correlation between IGF-I and Hb (r = 0.41, p = 0.05). Most of the patients (90%) had negative scores for IGH-I SDS values, with 40% below –2 SDS (Table II). IGF-I SDS correlated negatively with ferritin (r = –0.46, p <0.05). Cranial MRI scanning of the two patients with GH insufficiency (Pts. No. 17 and 18) revealed ferritin deposition in basal ganglia (Fig.1). Their LH and FSH levels were in the normal range [LH: 6 and 8 mIU/ml, FSH:8 and 9 mIU/ml respectively; normal: 2-12 mIU/ml]. The serologic tests of our patients revealed that, at diagnosis only two patients (10%) were seropositive for both anti-HbC and anti-HbS; none of the patients was positive for anti-HCV. Following the therapy, one patient was found to be positive for anti-HCV (Pt 20). Liver biopsy was performed in these three children and they were followed up. Table I__Patient Characteristics
*Decimal year. Table II__Laboratory Data of the Patients
Growth retardation has been reported to occur in most patients with beta-thalassemia major(1-4). Several mechanisms may be involved, including chronic anemia, iron overload, and endocrine abnormalities. Apart from hypogonadotrophism, defective IGF-I activity has been suggested as one of the causes of this growth failure, as significant suppression of GH is usually not seen(3,4). In our population, though transfusions were regular, pretransfusion Hb levels were suboptimal and some children were receiving only short time iron chelation therapy. Height SDS were negative, but only four patients (Pts. No. 11,18,19,20) had serious growth retardation. However, the height SDS values of our patients showed no statistically signifi-cant correlation with mean pretransfusion Hb, and serum ferritin levels. All patients but two had normal GH response to L-dopa stimulation, with peak GH response strongly correlated with height SDS. Most studies reported similar findings(1-4). Pintor et al. investigating an older population, found low GH responses to growth hormone releasing hormone (GHRH) and glucagon and held iron deposition in the hypothalamus and hypophysis responsible for GH insuffi-ciency(2). Martin et al. reported that the GH secretion increased in mice when ventro-medical hypothalamic nuclei were stimulated with electrical current(8). Through MRI scanning of our two GH insufficient patients, iron deposition was documented in basal ganglia. Whether these deposits interact with GHRH secretion remains to be established. Interestingly, some patients (Pts. No. 3,6,19) had supranormal basal GH levels. This was also reported elsewhere and was related to diminished somatostatin secretion(9,10). In general we found a tendency to low IGF-I levels and this was more striking in older patients. One of our patients (Pt. No. 20) was found to be positive for anti-HCV and chronic hepatitis and siderosis seen in the liver biopsy. Liver dysfunction could be contributing to her growth retardation. In our study population we did not found glucose intolerance or hypothyroidism (11, 12). We could document a relationship between IGF-I SDS and ferritin despite the limited number of our patients. This suggests that poor clinical control may be responsible for growth retardation. Its pathogenesis seems to be related to diminished IGF-I production, and in long standing cases, to diminished GH secretion. Better clinical control would possibly minimize growth retardation in these children. Contributors: AO and IA co-ordinated the study (design and interpretation) and drafted the paper. AY and CT participated in the data collection and drafting. Funding: None. Competing interests: None stated.
Fig. 1. MRI showing ferritin deposition in the basal ganglia.
|
![]()