|
|
Survey Indian Pediatrics 2001; 38: 263-266 |
|||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
The National Family Health Survey (1998-99): Childhood Mortality |
|||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
The National Family Health Survey (NFHS-2)(1) conducted in 1998-99 provides a comprehensive profile of population, health, and nutrition in India. The information was collected from a representative sample of approximately 90,000 ever married women aged 15-49 years drawn from all states of the country. A similar number of women were covered during the NFHS-1 in 1992-93(2), which provided a comprehensive demographic and health database for India. Infant and child mortality reflects a country’s socio-economic development. Therefore in the present communication some of the salient findings of the NFHS-2 with regards to trends and determinants of childhood mortality are presented.
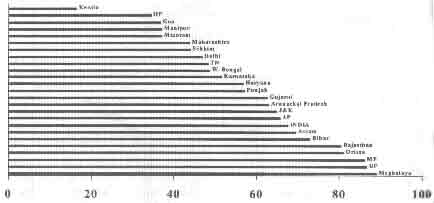
There has been a decline in all childhood mortality rates between the 4 years preceding NFHS-1 (1988-92) and NFHS-2 (1994-98). The Neonatal Mortality Rate (NMR) for India has declined from 48.6 to 43.4 per 1000 live births. Infant Mortality Rate (IMR) has declined from 78.5 to 67.6 per 1000 live births. The Child Mortality Rate (1-4 years) (4q1) has declined from 33.4 to 29.3 per 1000 children 1-4 years and the Under 5 Mortality Rate (U5MR) from 109.3 to 94.9 per 1000 live births. There is a 16% decline in the IMR in the 6-year interval between the two surveys, of which two-thirds of the decline has been contributed by the decline in NMR. During the 10 years preceding the NFHS-1, infant mortality rates declined by 16%; about 52% of this reduction was contributed by the decline in neonatal mortality rates. In contrast, during the 10 years preceding the NFHS-2, infant mortality rates declined by 13%; about 75% of this reduction was contributed by the decline in neonatal mortality rates. The increased proportional contribution of NMR to IMR reduction between 1984-92 and 1990-98 could suggest the possible contribution of strategies targeted towards reduction of neonatal mortality at the country level (e.g., the launch of the Child Survival and Safe Motherhood program in 1992-93). During the same 10-year period preceding NFHS- 1 and 2, the decline in child mortality was 11% and 8% respectively. Figure 1 depicts the IMR for the states of India (1994-98). There is a wide variation in the IMR across the states of India. The states of Meghalaya (89), Uttar Pradesh (87), Madhya Pradesh (86), Orissa (81), Rajasthan (80), Bihar (73) and Assam (70), have a higher IMR than the national average of 67.6 per 1000 live births. On the other hand, Kerala has the lowest IMR at 16.3 per 1000 live births. Inspite of the decline in the national infant mortality rates, several states have been observed to have a rise in IMR between 1988-92 and 1994-98. These include Arunachal Pradesh (40 to 63.1), Goa (31.9 to 36.7), Jammu and Kashmir (45.4 to 65), Madhya Pradesh (85.2 to 86.1), Meghalaya (64.2 to 89.0), Nagaland (17.2 to 42.1), Punjab (53.7 to 57.1), and Rajasthan (72.6 to 80.4). It is difficult to comment as to whether the increase is genuine or a result of sampling and survey methodologies.
Sex and Place of Residence: The neonatal and infant mortality rates are lower in females than in males both in urban and rural areas. The female child mortality rates (the number of female deaths at age 1-4 years per 1000 female children surviving to age 1 year) is one and a half times the male child mortality rates in both urban and rural areas. The female disadvantage is much more severe in rural than in urban areas. This probably suggests a gender bias and a neglect of the needs of the girl child. The disadvantage of the rural child is evident in the higher infant and neonatal mortality rates in rural than in urban areas in either sex (Table 1).
Birth Interval: Birth interval was observed to be indirectly proportional to infant and child mortality rates. At birth intervals of < 24 months the NMR was 71.7 and IMR was 109.5. However, when birth interval increased beyond 48 months NMR declined to 24.1 and IMR to 38.5. Medical Care During Pregnancy and Delivery: It is a known fact that adequate care during pregnancy and delivery can directly influence neonatal mortality and secondarily the infant mortality too. The neonatal mortality rate for children whose mothers had received no antenatal or intra-partum care (53.6) was almost one and a half times the mortality amongst children whose mothers had received some antenatal/intrapartum care (35.8), and two and a half times that amongst mothers who have received adequate care. Infant mortality rates were also about one and a half times higher amongst mothers receiving no care than mothers who had received some care during pregnancy and delivery.
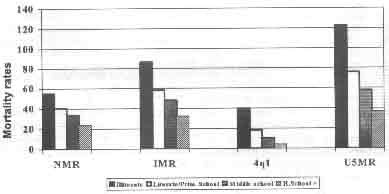
Maternal Education: Figure 3 depicts the association between maternal education and child mortality rates. All components of child mortality are observed to decline with increasing maternal education. All child mortality rates are higher amongst illiterate mothers compared to mothers who had completed high school education. The infant mortality rate for children of illiterate mothers is one and a half times the rate for children of mothers who are literate, and is two and a half times the rate for children whose mothers have atleast completed high school.
Standard of Living: In household with low standard of living the neonatal mortality is two times, the post-neonatal mortality is three times and 1-4 year child mortality is five times that of households with high standard of living. These differences are more obvious in urban than in rural areas.
The childhood mortality trends show a declining trend in India, but they are not uniform across the country. Children born to mothers who are young or elderly, are grand multiparous women, illiterate, and have received inadequate antenatal/intrapartum care are at higher risk of death during their first five years of life than other children. Children in rural areas and coming from households with low living standards also are at increased risk of childhood mortality. Above all, being born a female bestows a major social disadvantage for 1-4 year childhood mortality. The country requires major thrusts in the areas of female literacy, female empowerment, and female socio-economic independence, if we have to witness major reductions in the under 5 mortality and its components in the near future.
| |||||||||||||||||||||||||||||||||||||||||||||||||||||||
![]()