A
pseudomeningocele
is formed when there is a tear in the dura with protrusion of the
leptomeninges and the subarachnoid space through the dural defect.
Classically, growing skull fractures caused by the pseudomeningoceles have
been described in the pediatric age group. However an intradiploic
location of these pseudomeningoceles is rare; and only twenty cases are
described(1-12). We present a four year old child who developed this
uncommon condition following a traumatic injury.
Case Report
A four-year-old boy had sustained a head injury when a
heavy object had fallen on him at the age of about one year. The child was
comatose for about a week following injury and had made gradual recovery.
Presence of a progressive occipital swelling caused the parents to seek
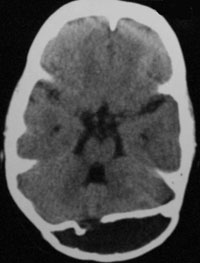
medical advice at 3 years of age. A plain CT head was performed at another
centre revealed a fracture in the inner table of the occipital bone with
the presence of an intradiploic pseudomeningocele (Fig 1a).
The outer table is seen to bulge outwards along this location but is
otherwise intact. The pseudomeningocele was misinterpreted by the treating
surgeon to be a calcified chronic subdural hematoma and a burr-hole
evacuation was attempted. However, as only cerebrospinal fluid was
obtained, the procedure was abandoned. One month following the procedure
the child developed a progressively enlarging swelling at the surgical
site which became more prominent when the child cried.
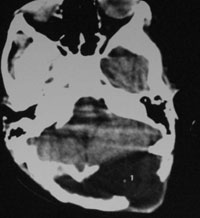
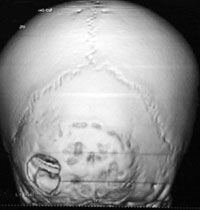
The child was referred to us in an unconscious state,
with a Glasgow coma score of E1V1M3. A repeat CT head showed gross
hydrocephalus with a subcutaneous CSF collection in the occipital region
which was communicating with the intradiploic pseudomeningocele through
the burr-hole (Fig 1b, 1c). An emergency
ventriculo-peritoneal shunt was placed, following which there was dramatic
recovery in the child’s sensorium along with resolution of the occipital
swelling. The child is presently on follow up and remains asymptomatic.
Discussion
An intradiploic pseudomeningocele is rare sequel of
skull fracture in the pediatric age group. The varied presentation of this
condition and the time span between the trauma and the formation of the
pseudomeningocele may result in misdiagnosis and in cases with concomitant
hydrocephalus, a ventriculperitoneal shunt may be considered as the first
line of treatment. Several mechanisms have been postulated for the
formation of growing skull fractures(5-7,11,12). It is widely agreed that
the leptomeninges prolapse through the bony defect in the fractured skull
bone and the pulsations of the normally growing brain prevents the
approximation of the dural as well as bony margins. Growing skull
fractures are uncommon in the occipital region because, the thickness of
the occipital bone and the overlying thick muscle cover, render it quite
resilient(8), nevertheless, in certain cases the inner table of the
occipital bone may be fractured leaving the outer table intact. A
concomitant dural laceration at the fracture site subsequently leads to
the progressive insinuation of the leptomeninges into the intradiploic
space. The growing brain provides a ball valve effect resulting in an
intradiploic leptomeningeal cyst. The mechanism of formation of the
intradiploic meningocele is essentially similar to that of the growing
skull fracture with some important differences. Due to their tendency to
develop in the occipital region it is hypothesized that an abundant muscle
cover buttressing the outer table of the occipital bone and the thickness
of the bone prevents the development of the classical lytic bony defect
associated with the growing skull fracture (8). Unlike growing skull
fractures, porencephaly, cystic encephalomalacia, ipsilateral ventricular
dilatation and seizures are not seen to be associated with an intradiploic
meningocoele(11).
The largest series of post traumatic intradiploic cysts
have been reported by Mahapatra, et al.(7). Of the 8 cases reported
by them 6 were in the parieto-oocipital region with 1 each in the frontal
region, parietal region and roof of the orbit. The time span between
injury and presentation ranged from one year to ten months. Patil, et
al.(10) described a variant of the intradiploic cyst with protrusion
of the parenchyma through the dural effect. They theorized that the
recoiling edges of the fractured bone might create the requisite negative
pressure for the leptomeninges and the cortex to be sucked into the
defect.
These cysts must also be differentiated from the
intradiploic arachnoid cysts which are probably congenital in origin, are
typically located within 3 cm of the midline in the occipital region, and
generally causes loss of the inner table of the skull and thinning of the
outer table without producing sclerotic bony margins. They are formed
because of an obstruction to the flow of CSF from the arachnoid
granulations into the venous system and usually present late in life with
local pain, swelling, seizures or neurological deficit (11).
Communicative type of hydrocephalus is usually
associated with the pseudomeningocele and may be caused by
intraventricular bleed at the time of the initial trauma. The treatment
for this condition ranges from a simple ventriculo-peritoneal shunting to
elaborate cranioplasty and dural repair.
Contributors: SM was involved in data collection
and preparation of the manuscript. He will act as guarantor of the study.
DA helped in manuscript writing.
Funding: Nil.
Competing interests: None stated.
References
1. D’Almeida AC, King RB. Intradiploic cerebrospinal
fluid fistula. Report of two cases. J Neurosurg 1981; 54: 84-88.
2. Dunkser SB, McCreary HS. Leptomeningeal cyst of the
posterior fossa. J Neurosurg 1971; 34: 687-692.
3. Goel A, Desai KI, Nadkarni TD, Muzumdar DP. An
unusual post-traumatic occipitocervical pseudomeningocele: case report.
Surg Neurol 2001; 56: 62-65.
4. Halliday AL, Chapman PH, Heros RC. Lepto-meningeal
cyst resulting from adulthood trauma: case report. Neurosurgery 1990; 26:
150-153.
5. Kumar R, Verma A, Sharma K, Rathi B, Malik V.
Post-traumatic pseudomeningocele of the orbit in a young child. J Pediatr
Ophthalmol Strabismus 2003; 40: 110-112.
6. Macmillan AI, Bartlett RJ, Brocklehurst G.
Intradiploic meningocoele in a 16-year-old girl. Br J Neurosurg 1997; 11:
359-361.
7. Mahapatra AK, Tandon PN. Post-traumatic intradiploic
pseudomeningocele in children. Acta Neurochir (Wien) 1989; 100: 120-126.
8. Martinez-Lage JF, Lopez F, Piqueras C, Poza M.
Iatrogenic intradiploic meningoencephalocele. Case report. J Neurosurg
1997; 87: 468-471.
9. Natale M, Bocchetti A, Scuotto A, Rotondo M, Cioffi
FA. Post traumatic retropharyngeal pseudomeningocele. Acta Neurochir (Wien)
2004; 146: 735-739.
10. Patil AA, Etemadrezaie H. Posttraumatic
intradiploic meningoencephalocele. J Neurosurg 1996; 84: 284-287.
11. Tizzard S, Gleave J, Antoun N, Macfarlane R.
Occipito-clival intradiploic meningocoele following skull fracture in
infancy. Br J Neurosurg 2001; 15: 188-190.
12. Turgut M, Ozcan OE, Karaman CZ. Post-traumatic
intra-osseous pseudomeningocele of the occipital bone. Australas Radiol
1998; 42: 262-263.