|
|
Guidelines for Practice Indian Pediatrics 2008; 45:203-214 |
|||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
Management of Steroid Sensitive Nephrotic Syndrome: Revised Guidelines |
|||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
Indian Pediatric Nephrology Group, Indian Academy of Pediatrics
Introduction Nephrotic syndrome is an important chronic disease in children. About 80% children with idiopathic nephrotic syndrome show remission of proteinuria following treatment with corticosteroids, and are classified as ‘steroid sensitive’. Most patients have multiple relapses, placing them at risk for steroid toxicity, systemic infections and other complications. A small proportion of patients who are not steroid sensitive (steroid resistant) are also at risk for similar complications and renal insufficiency. Most pediatricians would encounter few patients with nephrotic syndrome in their practice. They should be familiar with management of these patients and be aware of situations in which referral to a pediatric nephrologist is required. Long-term management of these patients should thereafter be a joint effort between the pediatrician and the pediatric nephrologist. Objectives Guidelines on the management of children with nephrotic syndrome were first formulated by the Indian Pediatric Nephrology Group in 2001(1). Since a number of studies on management of these patients have been published during the last 7 years, it was felt desirable to review the existing recommendations. Therefore, following a preliminary meeting in New Delhi (7 March 2007), a draft statement was prepared, circulated and reviewed by pediatric nephrologists across the country (Annexure I). The present document reflects the current opinion on management of patients with steroid sensitive nephrotic syndrome. Recommendations Important revisions in this document are listed in Table I. TABLE I Important Revisions in this Document
Definitions Nephrotic syndrome is characterized by heavy proteinuria, hypoalbuminemia (serum albumin <2.5 g/dL), hyperlipidemia (serum cholesterol >200 mg/dL) and edema(1,2). Nephrotic range proteinuria is present if early morning urine protein is 3+/4+ (on dipstick or boiling test), spot protein/creatinine ratio >2 mg/mg, or urine albumin excretion >40 mg/m2 per hr (on a timed-sample). Precise quantitative assessment of proteinuria, including 24-hr urine protein measurement is seldom necessary. Definitions for clarifying the course of nephrotic syndrome are shown in Table II. TABLE II Definitions Related to Nephrotic Syndrome
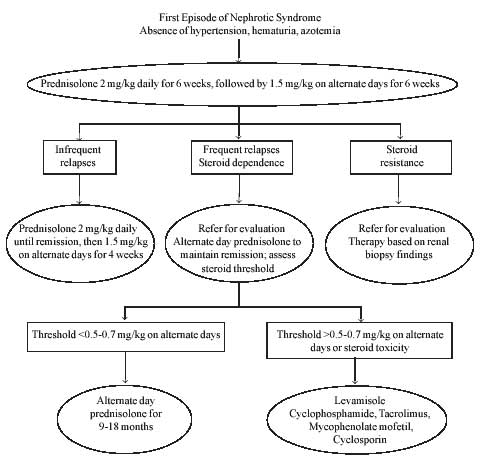
Initial Evaluation A detailed evaluation is necessary before starting treatment with corticosteroids. The height, weight and blood pressure should be recorded. Regular weight record helps monitor the decrease or increase of edema. Physical examination is done to detect infections and underlying systemic disorder, e.g., systemic lupus erythematosus, Henoch Schonlein purpura, etc. Infections should be treated before starting therapy with corticosteroids. Investigations recommended at the initial episode include: (i) urinalysis; (ii) complete blood count, blood levels of albumin, cholesterol, urea and creatinine. Estimation of blood levels of anti-streptolysin O and C3 is required in patients with gross or persistent microscopic hematuria. Appropriate tests are performed, if necessary, for associated conditions (e.g., chest X-ray and tuberculin test, hepatitis B surface antigen, antinuclear antibodies). Urine culture is not necessary unless the patient has clinical features suggestive of a urinary tract infection. Treatment of the Initial Episode Adequate treatment of the initial episode, both in terms of dose and duration of corticosteroids, is important. Evidence from multiple studies suggests that appropriate therapy at the first episode of nephrotic syndrome is an important determinant of the long-term course of the disease(3). Medication: The standard medication for treatment is prednisolone or prednisone. The medication is administered after meals to reduce its gastro-intestinal side effects. The use of methyl-prednisolone, dexamethasone, betamethasone, tri-amcinolone or hydrocortisone is not recommended. There is also limited evidence on the efficacy or benefits of therapy with deflazocort for nephrotic syndrome. Treatment regimen: Various treatment regimens have been used for the treatment of the initial episode of nephrotic syndrome. The International Study for Kidney Diseases in Children had originally recommended a regimen comprising of four-weeks each of daily and alternate day steroid therapy(4), which was used for almost three decades. Controlled studies later suggested that prolongation of initial steroid therapy for 12 weeks or longer is associated with significantly reduced risk for subsequent relapses. However, prolonged treatment with steroids is associated with a higher frequency of adverse events(3,5,6). The Cochrane Renal Group(3), on systematic analysis of the literature, recommends that the duration of initial prednisolone therapy should be for a minimum of 12 weeks. It further suggests that the benefits of sustained remission and reduction in relapse rates are superior if alternate-day treatment is not stopped abruptly at 12 weeks, but tapered over the next 2-4 months. It is emphasized that none of the studies included in this analysis was placebo-controlled, most lacked allocation concealment and were not powered to evaluate side effects of prolonged treatment(3). The debate regarding appropriate dose and duration of steroid treatment is not resolved. Other regimens are being examined that reduce the risk of relapse without increased side effects. Based on current evidence and opinion, the Group recommends that the initial episode of nephrotic syndrome be treated with prednisolone at a dose of 2 mg/kg per day (maximum 60 mg in single or divided doses) for 6 weeks, followed by 1.5 mg/kg (maximum 40 mg) as a single morning dose on alternate days for the next 6 weeks; therapy is then discontinued. The benefits and safety of prolonged initial steroid therapy, beyond 12 weeks, require confirmation from further studies. Treatment of Relapse The patient should be examined for infections, which should be treated before initiating steroid therapy. Appropriate therapy of an infection might rarely result in spontaneous remission, thereby avoiding the need for treatment with corticosteroids. Prednisolone is administered at a dose of 2 mg/kg/day (single or divided doses) until urine protein is trace or nil for three consecutive days. Subsequently, prednisolone is given in a single morning dose of 1.5 mg/kg on alternate days for 4 weeks, and then discontinued(1,5). The usual duration of treatment for a relapse is thus 5-6 weeks. Prolongation of therapy is not necessary for patients with infrequent relapses (see below). In case the patient is not in remission despite two weeks treatment with daily prednisolone, the treatment is extended for 2 more weeks. Patients showing no remission despite 4 weeks’ treatment with daily prednisolone should be referred for evaluation. Infrequent Relapsers Patients who have three or less relapses a year and respond promptly to prednisolone are managed using the aforementioned regimen for each relapse. Such children are at a low risk for developing steroid toxicity. Frequent Relapsers and Steroid Dependence Patients with frequent relapses or steroid dependence should be managed in consultation with a pediatric nephrologist. It is usually not necessary to perform a renal biopsy in these cases. Following treatment of a relapse, prednisolone is gradually tapered to maintain the patient in remission on alternate day dose of 0.5-0.7 mg/kg, which is administered for 9-18 months. A close monitoring of growth and blood pressure, and evaluation for features of steroid toxicity is essential. If the prednisolone threshold, to maintain remission, is higher or if features of corticosteroid toxicity are seen, additional use of the following immuno-modulators is suggested. (a) Levamisole is administered at a dose of 2-2.5 mg/kg on alternate days for 12-24 months(7-9). Co-treatment with prednisolone at a dose of 1.5 mg/kg on alternate days is given for 2-4 weeks; its dose is gradually reduced by 0.15-0.25 mg/kg every 4 weeks to a maintenance dose of 0.25-0.5 mg/kg that is continued for six or more months. Occasionally, it might be possible to discontinue treatment with corticosteroids. The chief side effect of levamisole is leukopenia; flu-like symptoms, liver toxicity, convulsions and skin rash are rare. The leukocyte count should be monitored every 12-16 weeks. (b) Cyclophosphamide is administered at a dose of 2-2.5 mg/kg/day for 12 weeks(10). Prednisolone is co-administered at a dose of 1.5 mg/kg on alternate days for 4 weeks, followed by 1 mg/kg for the next 8 weeks; steroid therapy is tapered and stopped over the next 2-3 months. Therapy with cyclophosphamide should be instituted preferably following remission of proteinuria. Total leukocyte counts are monitored every 2 weeks; treatment with cyclophosphamide is temporarily discontinued if the count falls below 4000/mm3. An increased oral fluid intake and frequent voiding prevents the complication of hemorrhagic cystitis; other side effects are alopecia, nausea and vomiting. The risk of gonadal toxicity is limited with a single (12 weeks) course of cyclo-phosphamide(7,10,11). The use of more than one course of this agent should preferably be avoided. In view of its toxicity, the use of chlorambucil, unless under close supervision, is not recommended. (c) Calcineurin inhibitors: Cyclosporin (CsA) is given at a dose of 4-5 mg/kg daily for 12-24 months. Prednisolone is co-administered at a dose of 1.5 mg/kg on alternate days for 2-4 weeks; its dose is gradually reduced by 0.15-0.25 mg/kg every 4 weeks to a maintenance dose of 0.25-0.5 mg/kg that is continued for six or more months. Occasionally, treatment with corticosteroids may be discontinued. Estimation of trough blood levels of CsA is required in patients with suspected non-compliance, unsatisfactory response or nephrotoxicity (increase in serum creatinine by 30% or more from the baseline)(12). Trough (12-hr) CsA levels should be kept between 80-120 ng/mL(12). Side effects of CsA therapy include hypertension, cosmetic symptoms (gum hypertrophy, hirsutism) and nephro-toxicity; hypercholesterolemia and elevated transaminases may occur. Estimation of blood levels of creatinine is required every 2-3 months and a lipid profile annually. A repeat kidney biopsy, to examine for histological evidence of nephrotoxicity, should be done if therapy with calcineurin inhibitors is extended beyond 2 years(12). Tacrolimus is an alternative agent, adminis-tered at a dose of 0.1-0.2 mg/kg daily for 12-24 months. Side effects include hyperglycemia, diarrhea and rarely neurotoxicity (headache, seizures). The use of tacrolimus is preferred especially in adolescents, because of lack of cosmetic side effects(13). Blood levels of creatinine and glucose should be estimated every 2-3 months. (d) Mycophenolate mofetil (MMF) is given at a dose of 800-1200 mg/m2 along with tapering doses of prednisolone for 12-24 months(7,14). The principal side effects include gastro-intestinal discomfort, diarrhea and leukopenia. Leukocyte counts should be monitored every 1-2 months; treatment is withheld if count falls below 4000/mm3. Choice of agent: The advantages of using these drugs should be balanced against their potential toxicity. There are few studies comparing one agent with another, but evidence for efficacy is strongest for cyclophosphamide and CsA. Levamisole has a modest steroid sparing effect and is a satisfactory initial choice for patients with frequent relapses or steroid dependence. Treatment with cyclophospha-mide is preferred in patients showing: (i) significant steroid toxicity, (ii) severe relapses with episodes of hypovolemia or thrombosis, and (iii) poor compliance or difficult follow up, where 12 weeks therapy might be possible to ensure than long-term compliance. Treatment with CsA or tacrolimus is recommended for patients who continue to show steroid dependence or frequent relapses despite treatment with the above medications(12). Either of these agents is effective in maintaining remission in most patients with steroid sensitive nephrotic syndrome. The chief concern with their use is nephrotoxicity, but with careful assessment of renal function, minimizing the maintenance dose and utilizing renal biopsies in those receiving prolonged therapy, this risk can be minimized. Recent case series(14) and a controlled trial(15) support the use of MMF as a steroid sparing agent. The lack of renal, hemodynamic and metabolic toxicity with this agent makes it an attractive alternative to calcineurin inhibitors. In some patients receiving therapy with levamisole, MMF and calcineurin inhibitors, treatment with prednisolone might be tapered and discontinued after 6-12 months. Some patients who respond to therapy with levamisole, MMF and calcineurin inhibitors may relapse once these medications are discontinued. Relapses during or following therapy with these agents are treated with prednisolone as described above. Failure of alternative medication: If a patient has two or more relapses over 6 months while on treatment with any of the above agents, its replacement with an alternative medication should be considered. A protocol summarizing the management of patients with steroid sensitive nephrotic syndrome is shown in Fig. 1.
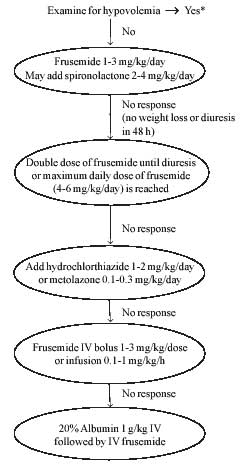
Supportive Care This forms an important aspect of managing children with nephrotic syndrome. Diet: A balanced diet, adequate in protein (1.5-2 g/kg) and calories is recommended. Patients with persistent proteinuria should receive 2-2.5 g/kg of protein daily(16). Not more than 30% calories should be derived from fat and saturated fats avoided. While salt restriction is not necessary in most patients with steroid sensitive nephrotic syndrome, reduction of salt intake (1-2 g per day) is advised for those with persistent edema. Salt should not be added to salads and fruits, and snacks containing high salt avoided. Since treatment with corticosteroids stimulates appetite, parents should be advised regarding ensuring physical activity and preventing excessive weight gain. Edema: Control of edema is an integral part of supportive care. Since treatment with corticosteroids usually leads to diuresis within 5-10 days, diuretics are avoided unless edema is significant. Diuretics should also not be given to patients with diarrhea, vomiting or hypovolemia. Patients with persistent edema and weight gain of 7-10% are treated with oral frusemide (1-3 mg/kg daily). Additional treatment with potassium sparing diuretics is not required if frusemide is used at this dose for less than one week. Patients requiring higher doses and prolonged duration of treatment with frusemide should receive potassium sparing diuretics, e.g., spironolactone (2-4 mg/kg daily). Blood pressure should be monitored frequently. A gradual reduction of edema, over one week, is preferred(16,17). Edema not responding to the above therapy should be managed in a hospital. A combination of a loop and thiazide diuretic, and/or a potassium sparing agent is occasionally necessary. For patients with refractory edema, a combination of diuretics and albumin infusion is used. Albumin (20%) is given as an infusion at a dose of 0.5-1 g/kg over 2-4 hr, followed by administration of frusemide (1-2 mg/kg intravenously). While infusion of albumin results in increased urine output, the effect is not sustained and repeated administration might be necessary. Albumin should be administered very cautiously in patients with renal failure, pneumonia or pulmonary edema due to its potential to increase the plasma volume. Patients receiving albumin should be observed for respiratory distress, hypertension and congestive heart failure. Refractory ascites interfering with respiration or associated with breaks in the skin may be removed by cautious paracentesis. A protocol for treatment of edema is shown in Fig. 2.
Patient and parent education: Long-term outcome of children with steroid sensitive nephrotic syndrome is satisfactory, with the majority in sustained remission and with normal renal functions by adolescence. A proportion of patients, especially those (i) with early onset of nephrotic syndrome, (ii) with a frequently relapsing course, and (iii) requiring treatment with alkylating agents or CsA may continue to show relapses beyond adolescence(18). Parents should be reassured that despite a relapsing course, progression to end stage renal failure necessitating dialysis or transplantation is extremely rare. Parental motivation and involvement is essential in the long-term management of these children. They should be provided information about the disease, its expected course and risk of complications. The following are emphasized: (a) Urine examination for protein at home using dipstick, sulfosalicylic acid or boiling test. The examination should be done every morning during a relapse, during intercurrent infections or if there is even mild periorbital puffiness. The frequency of urine examination is reduced, to once or twice a week, during remission. The importance of detecting relapse before development of significant edema is stressed. (b) Maintain a diary showing results of urine protein examination, medications received and intercurrent infections. (c) Ensure normal activity and school attendance; the child should continue to participate in all activities and sports. (d) Since infections are an important cause of morbidity, patients should receive appropriate immunization and other measures for protection. Other medications: The use of antacids or histamine receptor antagonists (e.g., ranitidine) is not necessary, unless there are symptoms of upper gastrointestinal discomfort. Long-term calcium supplementation (calcium carbonate, 250-500 mg) is necessary if the patient receives more than 3 months treatment with prednisolone(19). Patients with steroid sensitive nephrotic syndrome do not usually require medications for hyperlipidemia, since lipids normalize following remission. Immunization: Parents should be advised regarding the need for completing the primary immunization. Administration of some vaccines, e.g., hepatitis B, measles-mumps-rubella or meningococcal vaccines may rarely precipitate a relapse. Patients receiving prednisolone at a dose of 2 mg/kg/day or greater, or total 20 mg/day or greater (for patients weighing >10 kg) for more than 14 days are considered immunocompromised(20). Such patients should not receive live attenuated vaccines; inactivated or killed vaccines are safe(20). Live vaccines are administered once the child is off immunosuppressive medications for at least 4 weeks. If there is a pressing need, these vaccines may be given to patients receiving alternate day prednisolone at a dose less than 0.5 mg/kg. All children with nephrotic syndrome should receive immunization against pneumococcal infections(21). It is important to note that not all pneumococcal serotypes are included in the vaccines and that antibody levels may decline during a relapse. Previously vaccinated children may, there-fore, develop pneumococcal peritonitis and sepsis. The Expert Group endorses the recommendations of the Immunization Committee of the Indian Academy of Pediatrics(22). The Committee recommends 2-4 doses of the heptavalent conjugate pneumococcal vaccine for children below 2 yr of age. For previously unimmunized children between 2-5 yr old, a priming dose of the conjugate vaccine should be followed 8 weeks later, by a dose of the 23-valent polysaccharide vaccine. Children older than 5 yr require only a single dose of the polysaccharide vaccine. The vaccine should be given during remission, preferably when the child is not receiving daily prednisolone. Revaccination after 5 yr is considered for children (<10-yr-old) with active nephrotic syndrome. Patients in remission and not on immuno-suppressive therapy should receive the varicella vaccine. One dose is recommended for children between 12 months and 12 yr of age, and 2 doses separated by an interval of at least 4 weeks for children 13 yr or older(23). Kidney Biopsy Children with idiopathic nephrotic syndrome not having hematuria, hypertension or impaired renal function are treated with corticosteroids without requiring a kidney biopsy. A biopsy is usually not necessary in patients with frequent relapses or steroid dependence before starting treatment with levamisole, cyclophosphamide or MMF, but should be performed before therapy with calcineurin inhibitors. A biopsy is required to identify the underlying renal disease in certain cases (Table III). TABLE III Indications for Kidney Biopsy
Kidney biopsies must be performed by experts with experience in the procedure. Centers that perform kidney biopsies should have facilities for evaluation of the specimens by light and immuno-fluorescence microscopy. Referral to Pediatric Nephrologist Indications for referral of patients are given in Table IV. The care of these patients should be a joint collaboration between the pediatrician and pediatric nephrologist. TABLE IV Indications for Referral to a Pediatric Nephrologist
Complications Patients with steroid sensitive nephrotic syndrome are at risk for certain complications, early detection of which is necessary. Infections: Children with nephrotic syndrome are susceptible to severe infections, which need prompt treatment. Common infections include peritonitis, cellulitis and pneumonia. Viral and bacterial infec-tions may occasionally precipitate relapses in patients previously in remission. The clinical features and management of common serious infections are summarized in Table V. TABLE V Clinical Features and Management of Infections*
*Supplemental stress doses of hydrocortisone or prednisolone are usually necessary Varicella may be a severe illness in patients with nephrotic syndrome receiving corticosteroids or other immunosuppressive drugs. Susceptible patients (those unimmunized or with no history of varicella) who are exposed to a case of chickenpox should therefore receive a single dose of varicella zoster immunoglobulin, within 96 hr of exposure to prevent or lessen the severity of the disease(17). Since, this preparation is expensive and not easily available, a single dose of intravenous immunoglobulin (400 mg/kg) may be used instead(23). However, no clinical data showing the effectiveness of the latter strategy are available. Patients who develop varicella should receive intravenous acyclovir (1500 mg/m2/day in 3 doses) or oral acyclovir (80 mg/kg/day in 4 doses) for 7-10 days(23). The dose of prednisolone should be tapered to 0.5 mg/kg/day or lower during the infection. Patients with nephrotic syndrome who are Mantoux positive but show no evidence of tuberculosis should receive prophylaxis with INH for six months(24). Those showing evidence of active tuberculosis should receive standard therapy with anti-tubercular drugs. Thrombosis: Children with nephrotic syndrome are at risk for venous and, rarely, arterial thrombosis(16,17). Reduced intravascular volume, immobilization, indwelling vascular catheters, aggressive diuretic use and puncture of deep vessels predispose to thrombus formation. Renal vein thrombosis is suspected in a patient with oligoanuria, hematuria or flank pain, especially following an episode of dehydration. Femoral and mesenteric arterial thrombosis may occasionally occur. Deep vein thrombosis of calf veins is less common in children but may lead to pulmonary embolism. Saggital sinus and cortical venous thrombosis may follow episodes of diarrhea and present with convulsions, vomiting, altered sensorium and neurological deficits. Ultrasonography, Doppler studies and cranial MRI are useful in confirming the diagnosis. Patients with thrombotic complications require urgent treatment. The treatment includes correction of dehydration and other complications, and use of heparin (IV) or low-molecular-weight heparin (subcutaneously) initially, followed by oral anti-coagulants on the long-term(16,17). There is no role for prophylactic treatment with anticoagulants in patients with hypoalbuminemia and edema. Hypertension: This may be detected at the onset of nephrotic syndrome or later due to steroid toxicity. Therapy is initiated with ACE inhibitors, calcium channel blockers or b adrenergic antagonists, keeping the blood pressure at less than the 90th percentile(25). Hypovolemic shock: This complication can occur due to unsupervised use of diuretics especially if accompanied by septicemia, diarrhea or vomiting. The diagnosis is suggested by moderate to severe abdominal pain, hypotension, tachycardia, cold extremities and poor capillary refill; hematocrit and blood levels of urea and uric acid are elevated. Management consists of rapid infusion of normal saline at a dose of 15-20 mL/kg over 20-30 minutes; this is repeated if clinical features of hypovolemia persist. Infusion of 5% albumin (10-15 mL/kg) or 20% albumin (0.5-1 g/kg) may be used in subjects who do not respond despite two boluses of saline. Corticosteroid side effects: Prolonged steroid therapy may be associated with significant side effects. Patients (if they can understand) and the parents should be explained about the side effects of the medications, including increased appetite, impaired growth, behavioral changes, risk of infections, salt and water retention, hypertension and bone demineralization. All patients should be monitored for cushingoid features and blood pressure; six-monthly record of height and weight, and yearly evaluation for cataract should be done. Patients on prolonged (>3 months) treatment with steroids should receive daily supplements of oral calcium (250-500 mg daily) and vitamin D (125-250 IU)(19). Steroids during stress: Patients who have received high-dose steroids for more than 2 weeks in the past year are at risk of suppression of the hypothalamo-pituitary-adrenal axis. These children require supplementation of steroids during surgery, anesthesia or serious infections(26). Corticosteroids are supplemented, as parenteral hydrocortisone at a dose of 2-4 mg/kg/day, followed by oral prednisolone at 0.3-1 mg/kg/day. This is given for the duration of stress and then tapered rapidly. Conclusions Recommendations on management of nephrotic syndrome, proposed in 2001, have been reexamined and revised based on systematic reviews, published studies and expert opinion of the members of the Indian Pediatric Nephrology Group. These guidelines are intended to familiarize physicians with principles of management of children with steroid sensitive nephrotic syndrome. Therapy needs to be individualized for each patient and optimal care will be achieved by combined inputs of the primary pediatrician and pediatric nephrologist. Further revisions of these guidelines, indicating best current practice, shall be periodically necessary. Annexure I Members of the Review Committee Kamran Afzal, Jawaharlal Nehru Medical College, Aligarh; Indira Agarwal, Christian Medical College Hospital, Vellore; Vinay Agarwal, Max Hospital, New Delhi; Uma Ali, Bai Jerbai Wadia Hospital for Children, Mumbai; Sanjeev Bagai, Rockland Hospital, New Delhi; Arvind Bagga, All India Institute of Medical Sciences, New Delhi (Convenor); Sushmita Banerjee, Calcutta Medical Research Institute, Kolkata; Ashima Gulati, All India Institute of Medical Sciences, Delhi; Sanjeev Gulati, Fortis Hospital, New Delhi; Pankaj Hari, All India Institute of Medical Sciences, New Delhi (Secretary); Arpana Iyengar, St. John’s Medical College, Bangalore; OP Jaiswal, Sunder Lal Jain Hospital, New Delhi; Rupesh Jain, Ekta Hospital for Children, Raipur; M Kanitkar, Armed Forces Medical College, Poona; Mukta Mantan, Maulana Azad Medical College, New Delhi; Kamini Mehta, Lilavati Hospital & Research Center, Mumbai; Kumud Mehta, Jaslok Hospital & Research Center & Bai Jerbai Wadia Hospital for Children, Mumbai; BR Nammalwar, Kanchi Kamakoti CHILDS Trust Hospital, Chennai; Amitava Pahari, Apollo Hospital, Kolkata; Saroj K Patnaik, No.12 Air Force Hospital, Gorakhpur; KD Phadke, St. John’s Medical College, Bangalore; PK Pruthi, Sir Gangaram Hospital, New Delhi; Abhijeet Saha, Government Medical College, Chandigarh; VK Sairam, Sri Ramchandra Medical College, Chennai; Jayati Sengupta, AMRI Hospital, Kolkata; Prabha Senguttuvan, Institute of Child Health, Chennai (Chairperson); Sidharth K Sethi, All India Institute of Medical Sciences, New Delhi; Mehul Shah, Apollo Hospital, Hyderabad; Jyoti Sharma, Bharti Vidyapeeth Medical College, Poona; RN Srivastava, Indraprastha Apollo Hospital, New Delhi; AS Vasudev, Indraprastha Apollo Hospital, New Delhi; Anil Vasudevan, St. John’s Medical College, Bangalore; and M Vijayakumar, Mehta Children’s Hospital, Chennai. Writing Committee Uma Ali, Arvind Bagga, Sushmita Banerjee, Madhuri Kanitkar, Kishore D Phadke, Prabha Senguttuvan, Sidharth Sethi and Mehul Shah, on behalf of the Indian Pediatric Nephrology Group.
|
![]()