|
|
Recommendations Indian Pediatrics 2007; 44:187-197 |
||||||||||||||
|
IAP Growth Monitoring Guidelines for Children from Birth to 18 Years |
||||||||||||||
|
Writing Committee V.V. Khadilkar Correspondence to Dr. V.V. Khadilkar, Consultant
Pediatric Endocrinologist, Hirabai Cowasji Jehangir Research Institute,
Jehangir Hospital, 32, Sassoon Road, Pune 411 001, India.
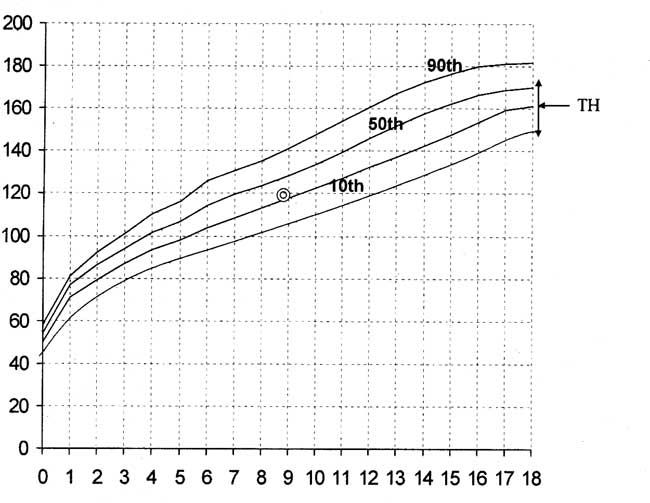
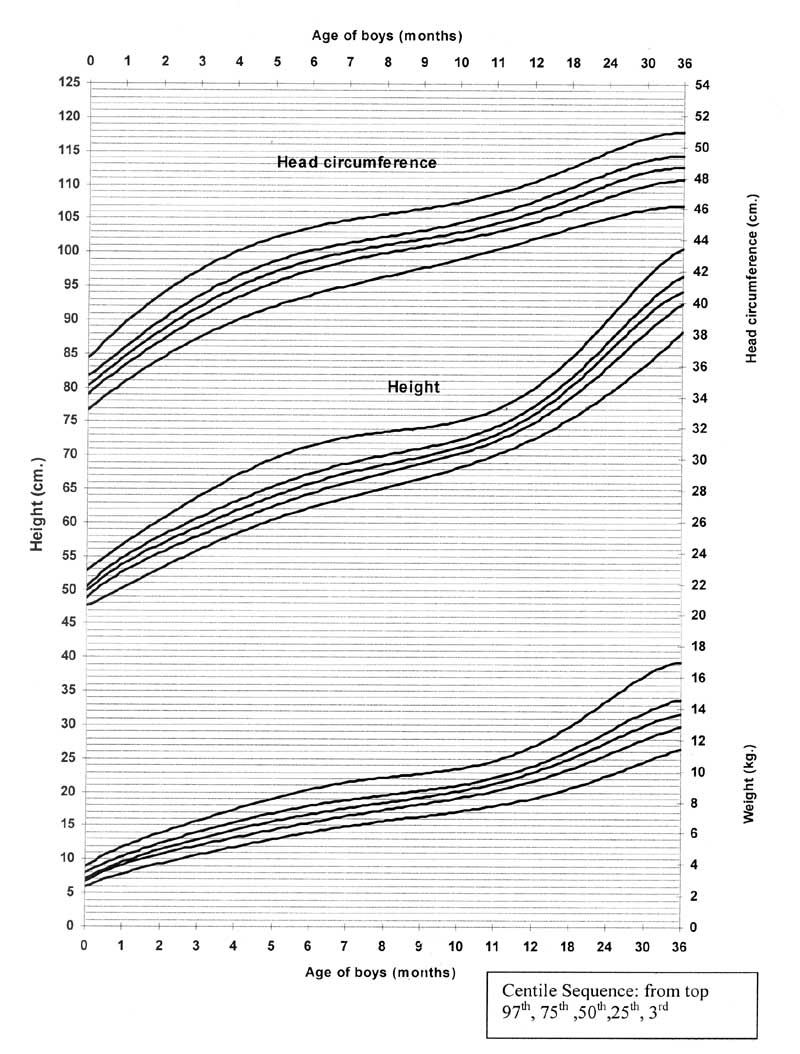
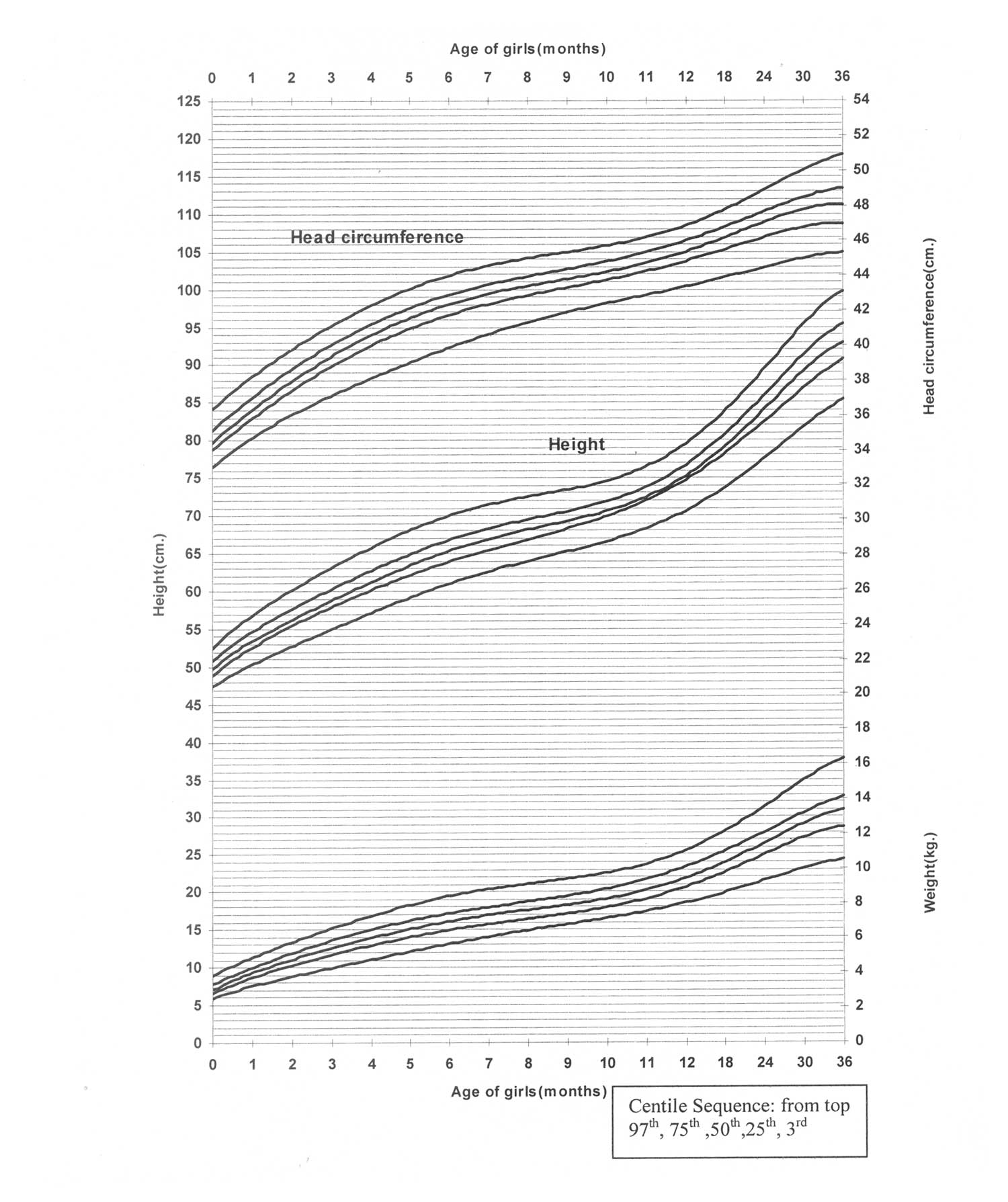
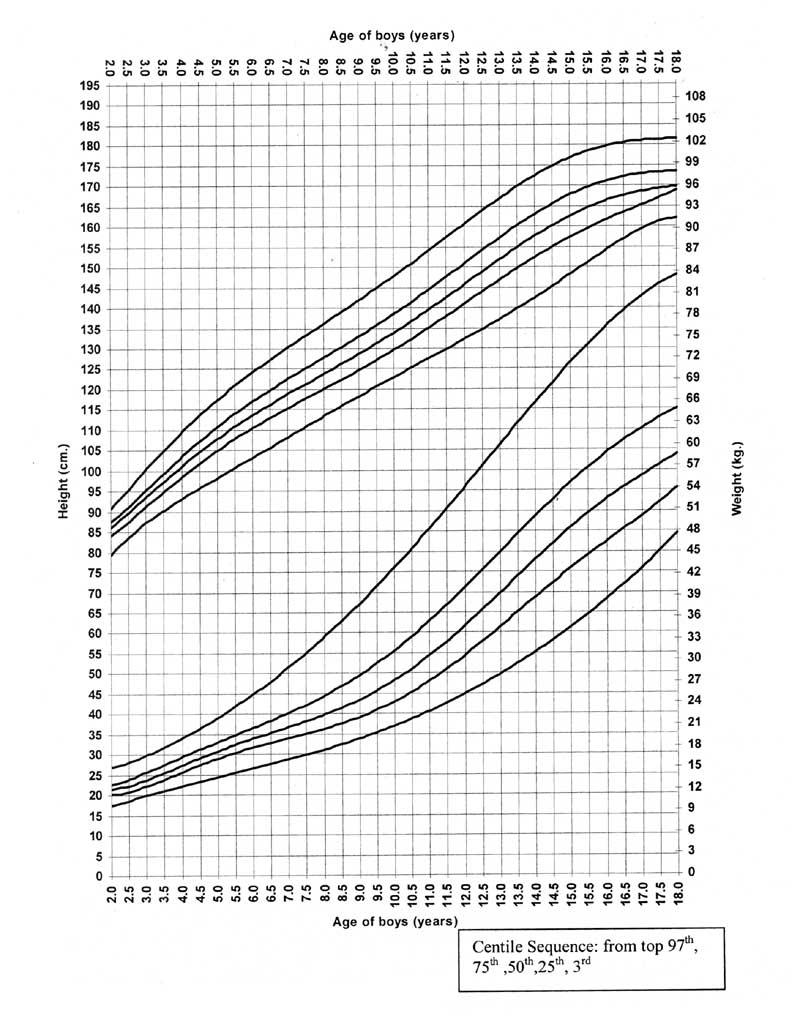
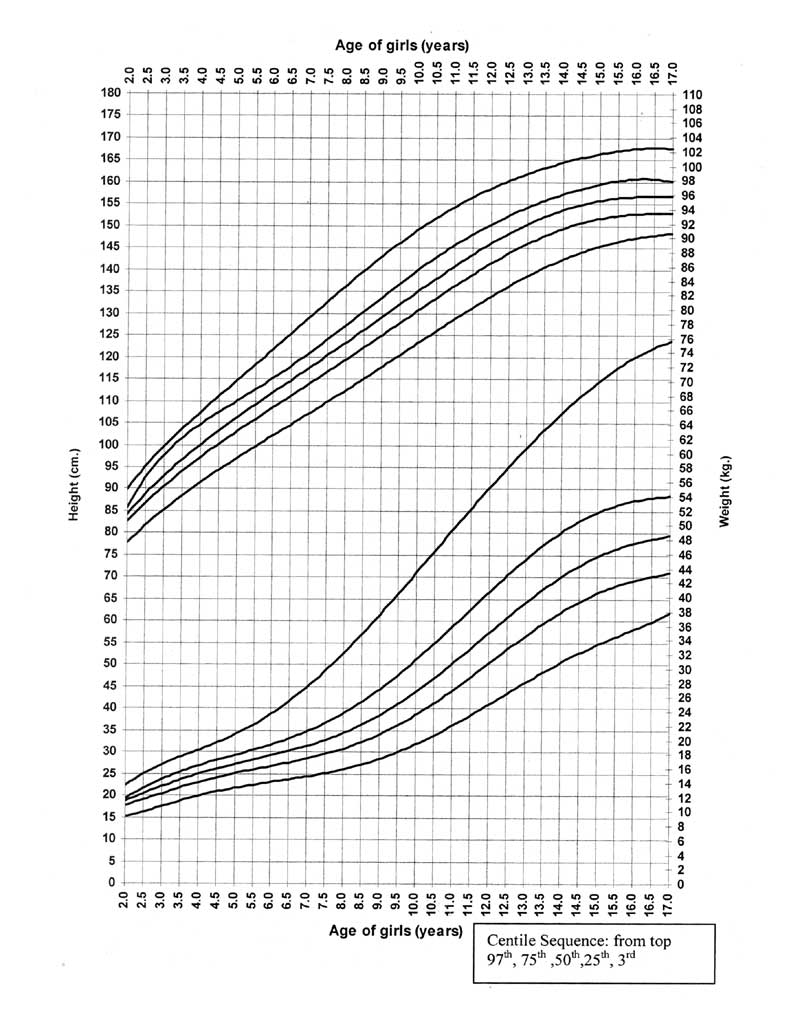
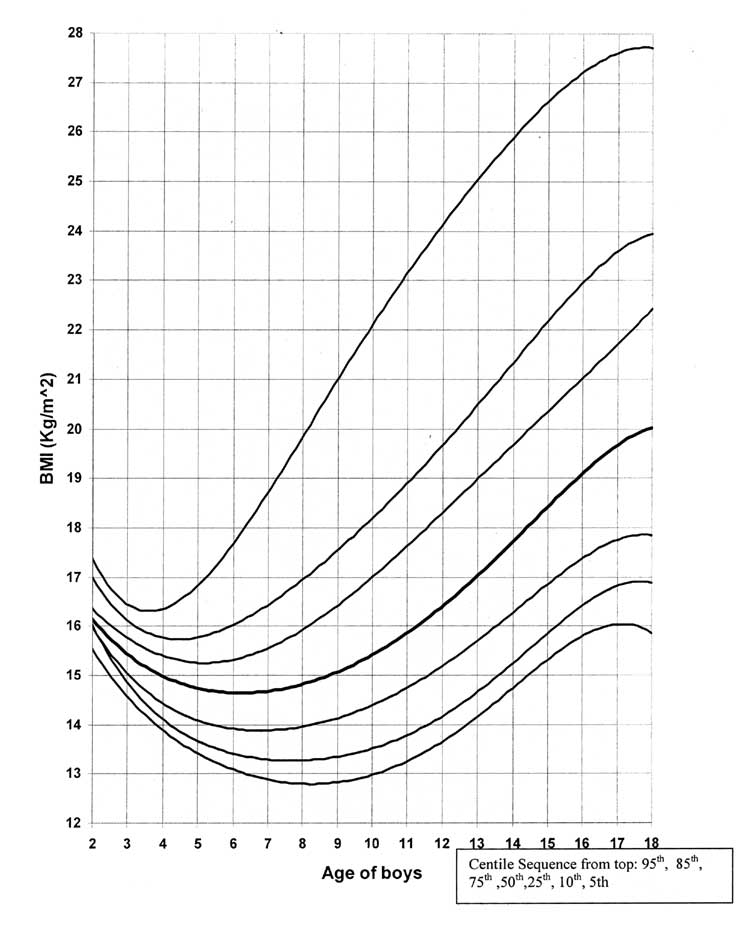
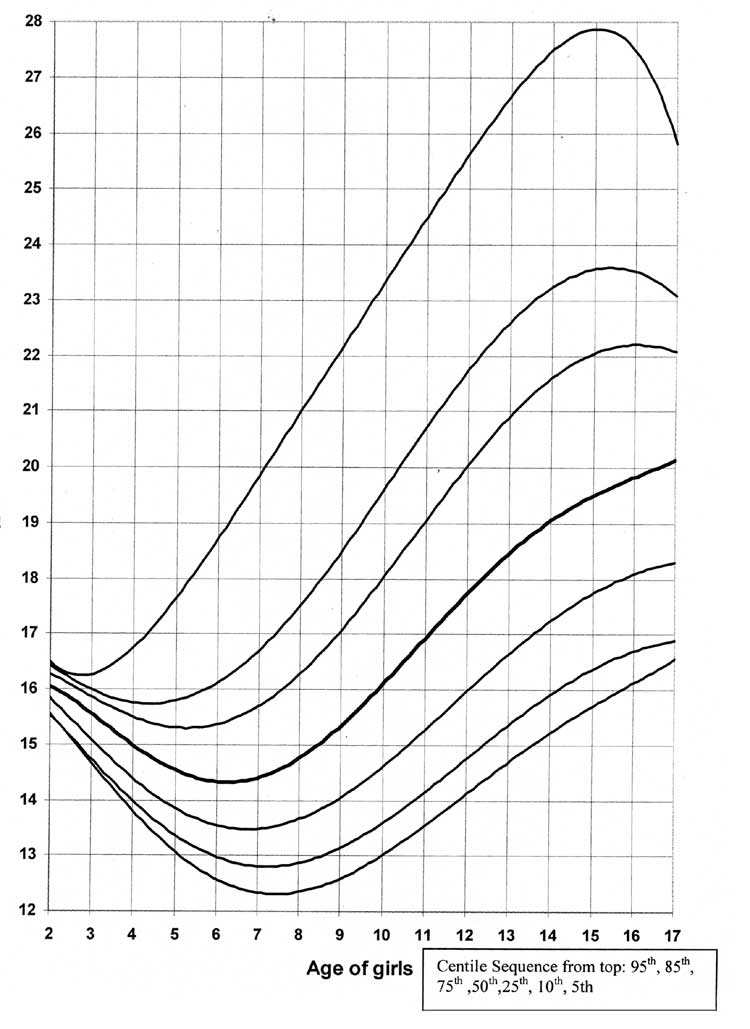
Introduction Growth Monitoring is a screening tool to diagnose nutritional, chronic systemic and endocrine disease at an early stage. It has been suggested that growth monitoring has the potential for significant impact on mortality even in the absence of nutrition supplementation or education(1). Experience in Tamilnadu, Maharashtra and other states in India indicates that individual growth monitoring of children is both feasible and extremely useful(2-4). Monitoring the growth of a child requires taking the same measurements at regular intervals, approximately at the same time of the day, and seeing how they change. A single measurement only indicates the child’s size at that moment. Currently, the Government policies for growth monitoring focus on children less than 5 years of age. Growth monitoring is one of the basic activities of the under 5 clinics where the child is weighed periodically at monthly intervals during the 1st year, every 2 months during the 2nd year and every 3 months thereafter up to the age of 5 to 6 years(5). Growth monitoring is viewed in most programs as an activity for weighing children regularly and plotting weight on growth charts to identify undernutrition (mostly severe Protein Energy Malnutrition) for feeding programs or to provide data on nutritional status(6). There are no national policies for growth monitoring beyond the age of 6 years. Growth monitoring differs greatly among pediatricians and often is not based on evidence. Hence, the Indian Academy of Pediatrics has made these consensus guidelines for growth monitoring as per IAP Action Plan 2006(members listed in Annexure I). This document gives a brief overview of aims and rationale for growth monitoring, growth charts, intervals for monitoring and criteria for referral. 1. Aims and Rationale Primary aims To identify children with growth deviation i.e., undernutrition and over nutrition and to identify diseases and conditions that manifest through abnormal growth. Secondary aims 1. To discuss health promotion related to feeding, hygiene, immunization and other aspects of the child’s health and behavior; education of parents to allay their anxiety about their child’s growth. 2. To sensitize pediatricians to use growth charts. 2. Which Charts to Use? Although the world’s children appear to follow a similar growth pattern, still there are variations due to ethnic, geographical, and regional factors giving different rates of maturation and adult stature. The final height of different ethnic groups is different, even accounting for secular trends. Thus for assessment, a national representative sample of population data are ideal as growth standards. The Indian Council for Medical Research (ICMR) undertook a nationwide cross sectional study during 1956 and 1965 to establish Indian reference charts. The measurements were made on children of the lower socio-economic class and hence cannot be used as a reference standard. The growth charts compiled by Agarwal, et al. (7,9) are based on affluent urban children from all major zones of India measured between 1989-91. These charts provide information on growth from birth to 18 years (unlike the new WHO standards providing data upto 5 years). Thus, in the present circumstances, these charts remain best option for growth monitoring in Indian children and are recommended for use by the Growth Monitoring Guidelines Consensus Meeting of the IAP (Figs. 2-7). At the community worker level, the continued use of the Government charts for monitoring of weight is recommended. The group also recommends use of (i) distance charts (presented from 3rd to 97th centiles) with data points taken at 6 monthly intervals; (ii) velocity charts to see the rate of growth at 6 monthly intervals; and (iii) BMI charts to help in guiding overweight (BMI for age more than 85th centile) and obesity (>95th centile) as per WHO recommendations. 3. How to Use Growth Charts 1. At the first visit the child’s name, date of birth and other details should be entered on the growth chart and the chart should be explained to the parents. This ensures that they are interested in it and are more likely to keep it properly and bring it at each visit. The growth chart should be kept with the parents in a plastic sleeve. 2. Measure the parents and make a note of their heights on the chart. Calculate the child’s target height and plot it at 18 years and mark it with an arrow on the growth chart. This represents the child’s projected height and his present height centile can be judged by tracing a line backward from this target height to child’s current height. The target range is produced by plotting two points 8 cms above and below the target height and this represents the 3rd and the 97th centile for that child. Taking those two points above and below the target height 97th and 3rd centiles are constructed by tracing lines backwards to match the current age (Fig. 1). 3. All the points on the growth chart should be marked only as dots and not circles around the dot. 4. The height and weight should be recorded (and head circumference till 3 years) and plotted on the chart. At all subsequent visits join the dot up to the previous dot. 5. Remind parents of the time for the next measurement. The group recommends continued use of Tanner staging of sexual maturity rating(10). For anthropometric measurements standard techniques as described by WHO should be adopted(11).
4. Recommended intervals and Parameters for Growth Monitoring (i) Birth to 3 years: Immunization contacts at birth, 6, 10 and 14 weeks, 9 months, 15-18 months may be conveniently used for growth monitoring. An additional monitoring visit at 6 months with opportunistic monitoring at other contacts (illness) is recommended. Normally growing babies should not be weighed more than once per fortnight under 6 months and no more than monthly thereafter, as this increases anxiety. After 18 months measurements are to be taken every 6 monthly. It is recommended that the height, weight and head circumference be measured upto 3 years of age. Penile length (PL) and testicular descent should be ascertained in the newborn period. (ii) 4 to 8 years: It is recommended that height and weight be measured 6 monthly during this period and BMI, PL and SMR should be assessed yearly from 6 years of age. (iii) 9-18 years: It is recommended that height, weight, BMI and SMR be assessed yearly during this period. 5. Criteria for referral (i) First three years • Length/height, weight or head circumference below 3rd percentile or above 97th percentile on growth chart. • Crossing of two major percentile lines (upward or downward) e.g., going from above 75th percentile to below 50th percentile on height or weight chart. • A child below or above mid parental range for height/length (see calculation for target height range in Fig. 2) • Weight loss or lack of weight gain for a month in the first 6 months. • Absence of weight gain for 2-3 months from 6-12 months of age. • Micropenis. • Unilateral or bilateral undescended testis. • Ambiguous genitals. (ii) Three to nine years • Length/Height below 3rd percentile or above 97th percentile on growth chart. • Crossing of two major percentile lines (upward or downward) e.g., going from above 75th percentile to below 50th percentile on height or weight chart. • A child below or above mid parental range for height (See calculation for target height range in Fig. 1). • BMI over the 85th percentile at all ages. • Rate of growth less than 5 cm/year. • Girls with axillary, pubic hair growth or breast budding before 8 years and boys with axillary, pubic hair growth, genital growth or and testicular enlargement before 9 years. • Children with craniospinal irradiation or surgery for brain tumors. • Micropenis. (iii) Nine to eighteen years • Height below 3rd percentile or above 97th percentile on growth chart. • Crossing of two major percentile lines (upward or downward) e.g., going from above 75th percentile to below 50th percentile on height or weight chart. • A child below or above mid parental range for height (Fig.1). • BMI over the 85th percentile at all ages. • Arrest at the same stage of puberty for more than 2 years. • Micropenis. • Unilateral or bilateral Gynecomastia in boys. • Hirsuitism and Menstrual irregularities in girls. • Delayed puberty that is girls with no breast budding by 14 years or no menarche by 15 years and boys with no signs of puberty by 16 years.
6. Epilogue Rate of growth of children is one of the finest indicators of the health of a community. Growth monitoring followed by suitable action prevents illness, malnutrition and even death. It provides reassurance about child’s health and prevents parental anxiety. On community and national level it helps identify children at risk of morbidity and mortality. It thus helps in implementation of national programmes for nutritional and medical interventions like supplementary feeding, foods to vulnerable group, underprivileged school children, etc. It is also a method to evaluate programs for improving child health and nutrition and can form the basis for policy making. Through growth monitoring mothers, family and community can be guided about the importance of nutrition in child growth and survival, ultimately resulting in better child rearing practices. The Indian Academy of Pediatrics thus urges all its members to perform regular Growth Monitoring. For details please refer to www.indianpediatrics.net and www.iapindia.org
Annexure I Chairperson: Dr. Nitin K. Shah, Conveners: Dr. Khadilkar V.V., Members 1. Dr. Khadilkar A.V., 2. Dr. Deepak Ugra, 3. Dr. Naveen Thacker, 4. Dr. Kamlesh Srivastava, 5. Dr Anju Seth, 6. Dr. Anju Virmani, 7. Dr. Chourjit Singh, 8. Dr. Dev Agarwal , 9. Dr. Kailash Agarwal, 10. Dr. Meena Desai, 11. Dr. Nalini Shah, 12. Dr. Palany Raghupathy, 13. Dr. Panna Choudhury, 14. Dr. Shabina Ahmed, 15. Dr. Shaila Bhattacharya, 16. Dr. Yeshwant Amdekar, 17. Dr. Vijayalakshmi Bhatia, | ||||||||||||||
|
References | ||||||||||||||
|
|
![]()