|
|
President's Page Indian Pediatrics 2007; 44: 169-171 |
||||||||||||||
|
Integrated management of neonatal and childhood illnesses: A new hope for child survival |
||||||||||||||
|
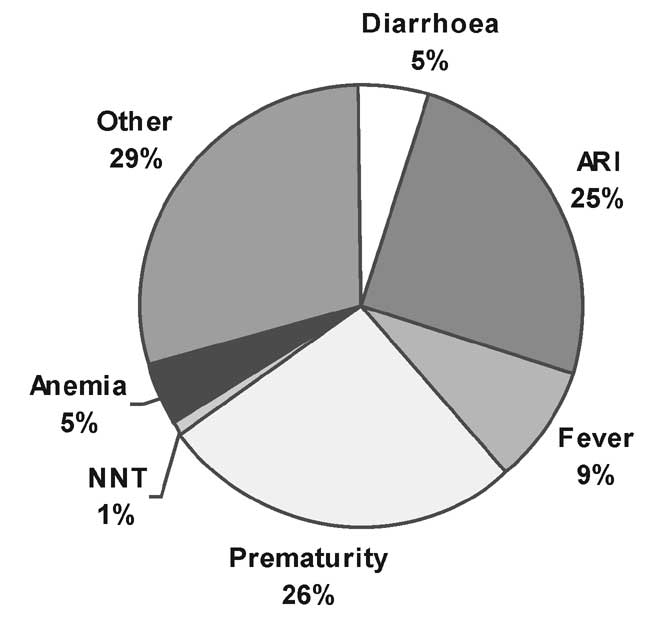
Early in this millennium, India and nations around the world committed themselves to achieve the Millennium Development Goals (MDG). Goal #4 aims to reduce under-5 mortality by two-thirds between 1990 and 2015. This means reducing under-five mortality to 36 per 1,000 live births and the Infant Mortality Rate (IMR) to 2711000 live births. Today, while there have been encouraging signs, India's Infant Mortality Rate (IMR) remains unbearably high at 58 per 1,000 live births (SRS 2004). We are behind in our challenge to meet this goal and must increase our efforts. The most challenging part of infant mortality, we all know, is the large proportion of newborn deaths, contributing to an estimated 64% of all infant deaths, mostly in the first week of life. Mortality rate in the second month of life is also higher than at later ages. In short, to achieve this goal, India needs extra emphasis to save newborns. The most common causes of infant and child mortality in developing countries including India are perinatal conditions, acute respiratory infections, diarrhea, malaria, measles and malnutrition (Fig. 1) These are also the commonest causes of morbidity in infants and young children.
Integrated Management of Childhood Illness (IMCI): The global strategy Developed during the mid-1990s by the WHO, UNICEF and other agencies, the global IMCI strategy focused primarily on the most common causes of child mortality diarrhoea, pneumonia, measles, malaria and malnutrition, illnesses affecting children aged 1 week to 2 months and 2 months to 5 years, including both preventive and curative elements to be implemented by families and communities as well as by health facilities. Following an algorithmic approach health providers are (re)trained to address a sick child in a systematic manner to address several medical conditions that often co-exist rather than only the main presenting symptom - which is often the case when child health programmes are implemented in a vertical fashion. For instance, all children, during an IMCI consultation are screened for malnutrition and assessed for immunization status, and given age appropriate feeding advice and immunization services. Integrated Management of Neonatal and Childhood Illnesses: The Indian adaptation In India, the "IMCI" strategy has been adapted by experts including representatives of the Indian Academy of Paediatrics giving central thrust to neonatal care component, the most critical period affecting infant mortality in India. This adapted version of IMCI was renamed as IMNCI (Integrated Management of Neonatal and Childhood Illnesses). The main adaptations to the package were: (i) Inclusion of first 7 days of life in the algorithms; (ii) 50% of training time for focussed on young infants (0-2 months); (iii) Adjustments of case management protocols consistent with current policies of the MoHFW, DWCD, and NVBDCP; and (iv) Adding home-based care of young infants by trained front-line workers (A WW and ANMs). The incorporation of home visits in India’s adaptation of IMNCI is an exciting innovation to bring the health system to the community level. Trained front-line workers extend quality inputs of the health system to household; helping to prevent illness’ and ensuring timely referral to a health facility for severe cases, During home visits, all newborns are assessed, any problems are identified and referred if necessary, and mother are taught ways to prevent illnesses and counselling to practice exclusive breastfeeding, keeping baby warm, and other essential newborn care, During these visits, mothers are also taught to keys signs of illnesses -when and where to seek timely caret (Table 1). TABLE I Specific Elements of IMNCI Clinical Protocols
Components of IMNCI implementation 1. Improving skills of health and front-line workers: IMNCI is skill based training. The training is based on a participatory approach, combining classroom sessions with hands-on clinical sessions (50% of training time) in both facility and community settings. Two categories of training are included, one for medical officers and pediatricians and a second for front-line functionaries including ANMs and Anganwadi Workers (A WWs). 2. Improving the health system: Trained workers need a functioning health system to be able to use their new found skills effectively. Facilities, drugs, and referral mechanisms need to be established in order to create the enabling environment for saving infants and newborns. 3. Improving of family and Community practices: Counseling of families and creating awareness among communities on newborn and childcare and early care seeking is an important component of IMNCI. 4. Collaborating with other departments, sectors: mplementation of IMNCI in an effective way in any district is possible only with the total involvement of ANM and Anganwadi workers of ICDS, and grassroot functionaries of other sectors. Community ownerships and participation is of paramount importance. Therefore, active involvement of PRI, self help groups and women’s groups is a must. The vital role of IAP to advance child survival IAP extends its full support for IMNCI approach for child survival. IMNCI training in the country at present is targeting the health care providers in public health system while present community behaviour pattern in rural India suggests that three fourth of population initially seek help of the private sector when they fall sick. Unless this large sector of private practitioners are brought into the IMNCI fold, we will never succeed. IAP can play a very important role here. IAP has planned a series of initiatives for IMNCI scaling up in our country. We plan to sensitize all 16000 IAP members about IMNCI approach by sending a book on IMNCI, by arranging one day orientation meeting for IAP members, by write ups in our publications and allotting slots in our conferences on IMNCI. IAP will come up with some innovative ideas for creating new packages suitable for training of private Practitioners. IAP vision 2007 aims to create District Resource Persons and nodal centres for training of IMNCI at district level in 2007. We will also utilize lAP Telemedicine and tele-education network for orientation and training on IMNCI. In long term it is very important that pre-service IMNCI training should be introduced in our country. We are planning to review guidelines on undergraduate and post graduate pediatric teaching in 2007 and we will examine feasibility of including IMNCI in pediatric curriculum. In a meeting held recently we have taken responsibility of holding planning meeting on acceleration of Pre-Service IMNCI in states of Assam, Andhra Pradesh, Delhi, Himachal Pradesh, lharkhand and Uttaranchal in year 2007. As the largest professional body constituting of pediatricians from all over the country, we must share our skills and our commitment to children by contributing to our country’s efforts to scale-up IMNCI. By joining hands, the skills to save newborn lives, to improve the functioning of the health system, and to educate mothers and families about child care practices can be accelerated for child survival. We have a golden opportunity in front of us. I would encourage all of us to learn about the algorithms devised under IMNCI. In addition, we are called upon in each of the districts where IMNCI is being implemented to contribute our expertise towards the rollout. Specific contributions that are being made, include support for the clinical aspects of IMNCI, opening the doors of our facilities to those who are learning IMNCI and providing facilitation of clinical training sessions. In many instances, members of IAP have also contributed to the coordination and oversight of IMNCI implementation. Finally, we are contributing to the improvements of the health system, continuing to strengthen and improve the quality of care in our institutions towards a more comprehensive approach to care for the chilren–ensuring that sick children referred to our care in a timely fashion receives the best possible chance at survival. The country is looking at us with expectant eyes. Come, let us answer their call. Naveen Thacker, |
![]()