First description of Fanconi’s anemia (FA) dates back
to 1927, where Fanconi described three brothers who had pancytopenia and
birth defects(1). Since then more than 1000 cases of Fanconi’s anemia
have been reported in the world literature(2). However of these only 9
cases were identified in the first month of life.
Case Report
A 36 week, 1380 grams, growth restricted male
neonate, born to a third gravida mother, with uneventful antenatal and
intrapartum period, was admitted to our NICU on day one of life.
Examination of the newborn revealed microcephaly, a small triangular
facies, bi-lateral anopthalmos, hypertelorism, depressed nasal bridge,
high arched palate, low set ears, webbed neck, widely spaced nipples,
bilateral undescended testis, radially curved left forearm and
hypoplastic biphalangial thumb attached to the palm by thin thread like
pedicle. Baby had an ecchymotic patch below left eyelid. No café au lait
spots were noted. Skeletal roentogenic survey revealed, left hypoplastic
radius, hypoplastic two phalanges of left thumb, curved ulna and
cervical hemivertebrae. Hematologic profile revealed significant
thrombocytopenia - Platelet count 40,000/cmm. Hemoglobin, red blood cell
morphology and white blood cell count were within normal limits.
Mother’s platelet count was normal. Bone marrow aspiration was a dry
tap.
Cytogenetic studies were performed on peripheral
blood lymphocyte cultures stimulated with Phytohemagglutinin (PHA)
induced with Mitomycin C (MMC) (40 ng/mL). Chromosomal preparations were
obtained using standard procedure and were subjected to GTG banding.
Chromosomal analysis revealed a high frequency of chromo-somal breakage
(6.0/metaphase) compared to control cultures (0.5/metaphase) (Fig. 1).
Cultures without MMC induction showed no chromosomal damage. The newborn
was diagnosed as a case of Fanconi’s anemia. Chromosomal analysis of sib
and parents revealed normal karyotype. In view of poor long-term
prognosis, parents refused any further treatment and baby was discharged
against medical advice on 15th day of life.
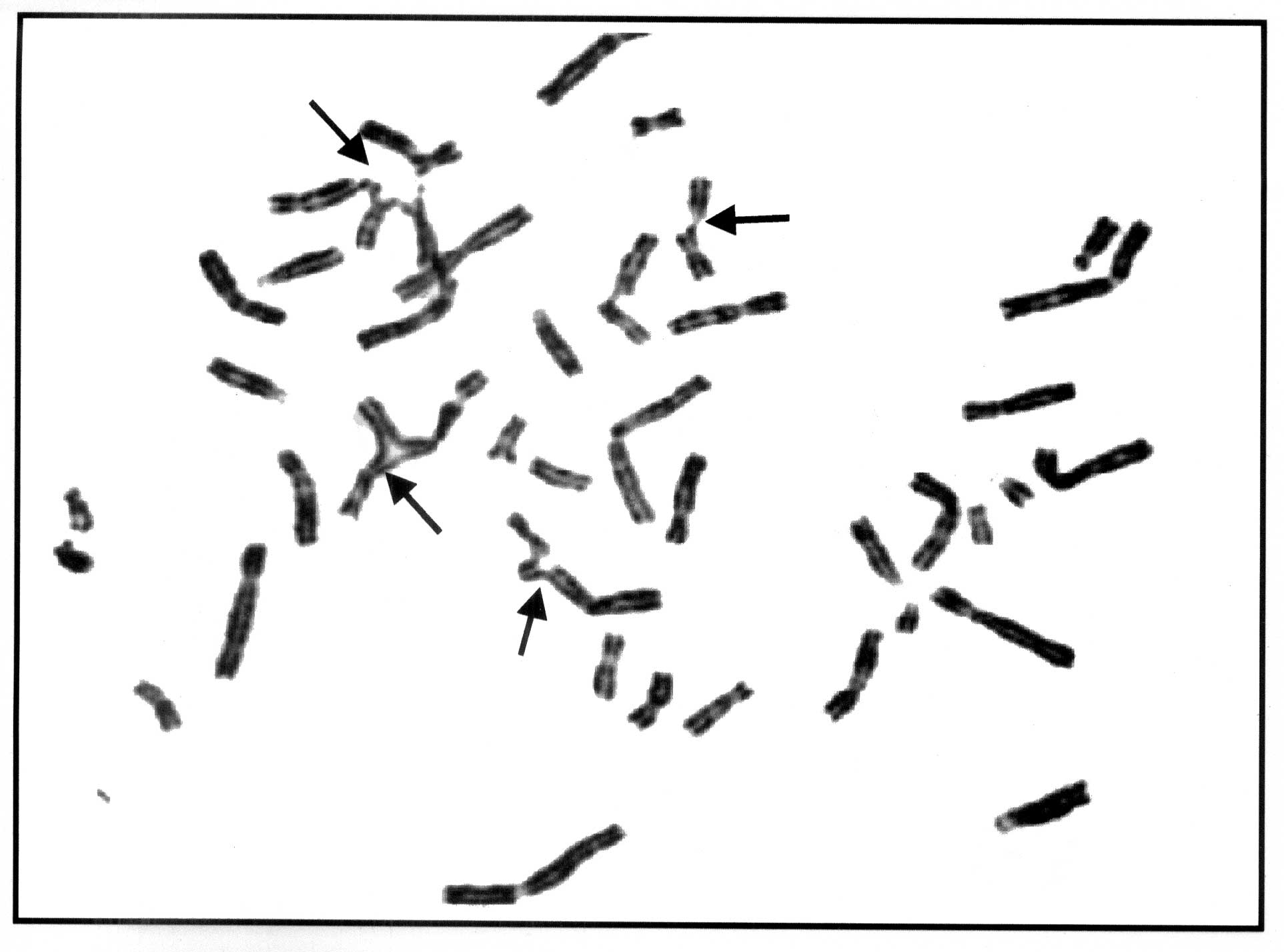 |
| Fig. 1.
Metaphase showing chromosome breakage and radial forms. |
Discussion
Diagnosis of Fanconi’s anemia (FA) is based on the
characteristic chromosomal breaks following clastogenic stress; the
presence of physical anomalies or aplastic anemia is not required for
diagnosis(2).
Physical anomalies described in FA involve almost all
the systems(2). ‘Classic’ phenotype of FA includes, short stature,
abnormality of the thumbs, microcephaly, café au lait and hypopigmented
spots and a characteristic facial appearance (a broad nasal base,
epicanthal folds, and micrognathia). FA newborns commonly have
hypogonadism and renal malformations(2,3). Radial ray
abnormality is the most common physical abnormality noted in the
patients with FA during infancy. Bilateral radial ray defect is more
common (78%) than unilateral (22%)(3). Hematologic abnormality at birth
is very rare(4).
Differential diagnosis considered in the present case
were, Thrombocytopenia– absent radius (TAR) syndrome, VATER / VACTERAL
syndrome, Trisomy 18 and Holt - oram syndrome.
TAR syndrome presents at birth with severe
thrombocytopenia with bleeding manifestations and radial ray defects(5).
Microcephaly, short webbed neck and skeletal anomalies noted in the
present case, though rare, have been reported in patients with TAR
syndrome (2,3). In FA, if the radii are affected, the thumbs are always
abnormal (absent / hypoplastic); in TAR, in which radii are absent, the
thumbs are always present(2). The present case had an abnormal thumb,
consistent with the diagnosis of Fanconi’s anemia.
FA has considerable overlap in the physical
abnormalities with VATER / VACTERAL syndromes. In a large series of FA
patients, 10% patients had three principal clinical features and
additional 20% patients had two major defects found in VATER
syndrome(6). Therefore, FA patient can be easily misdiagnosed as VATER/
VACTERAL syndrome. The present case had vertebral and limb defects.
VATER or VACTERAL syndromes are sporadic where as FA has 25% chance of
recurrence and misdiagnosis has severe consequences for genetic
counseling(7). Therefore it is recommended to rule out FA in patients
with suspected VATER / VACTERAL syndromes by chromosomal testing(3,6).
Holt-Oram syndrome has radial ray defects with
cardiac defects (100% cases). In the present case there were no cardiac
defects(5). Trisomy 18 can rarely have radial ray defects and eye
anomalies. However trisomy 18 has host of different physical
abnormalities and a typical facies(2). In the present case diagnosis of
FA could be established only after chromosomal breakage studies.
Diagnosis of FA requires high index of suspicion as
it presents with physical abnormalities involving multiple systems and
hematologic abnormalities at birth are extremely rare. Early diagnosis
in FA is very important as long term survival depends on the age of
onset of hematologic abnormalities or malignancies(8). If FA is
recognize in the preanemic phase, drugs and environmental insults
implicated in acquired aplastic anemia or malignancy can be avoided and
life span can be prolonged(2). Early diagnosis also offers options of
planning next pregnancy; as the umbilical cord blood can be used for
stem cell transplantation. Bone marrow or umbilical cord blood
transplantation from an HLA identical sibling is now considered the
treatment of choice for FA(3,7).
Acknowledgements are due to Dr. Nilima Kshirsagar,
Dean, Seth G.S. Medical College and K.E.M. Hospital, for permitting to
publish this article.
Contributors: TBP was involved in management of
patient, data collection, review of literature and drafting the
manuscript, RHU and RNN were involved in management of patient, concept
and design of the article and critical revision of the manuscript for
important intellectual content. VBR was involved in carrying out
cytogenetic studies and helped in preparation of manuscript.
Funding: None.
Competing Interests: None.
