|
|
Special Article Indian Pediatrics 2005; 42:233-244 |
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
All Slums are Not Equal: Child Health Conditions Among the Urban Poor |
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
Siddharth Agarwal From USAID-EHP Urban Health Program managed by CDM International Inc. Correspondence to: Shivani Taneja, Muskaan, 14, Nadir
Colony, Shamla Hills,
Introduction We only need to look around us to see ‘urbanization’–a constant growing phenomenon of increasing populations living in cities. This is a worldwide trend, but the increasing inability to respond to this situation has been noted more in low-income countries(1). In India, 28% of the total population was living in urban areas in 2001, with a future projection of about 50%, with 605-618 million by 2021-2025(2). Demographic trends show that while urban average growth rate stabilized at 3% over the past decade (1991-2001), the slum growth rate was double at 5-6%. An alarming feature of the urban population growth is the proportion of people living in poverty: official figures show 32%. Projections suggest while the urban population shall double in the next 10 years, the urban poor shall double in just 5 years(3). The above scenario has resulted in increased focus on urban populations. However, programs developed and implemented by agencies (NGOs, donors, government) that are external to the slum, are often not able to reach the neediest. Program, opportunities and resources are relatively easier accessed by the relatively better off groups among slum dwelling population. Issues of financial and institutional sustain-ability measurable by results, require patience and intensive efforts. This is more difficult with vulnerable groups, in a short program period. Consequently, such populations are left out of programs driven by short term targets. This paper describes the rationale for identifying the most vulnerable among the urban poor, while planning city level child health interventions. It also shows how standard programs successful in one slum do not bring about the same results in another area owing to differential vulnerability. The paper also describes an approach by which the urban poor can be identified and classified at different levels of health vulnerability. The differential health burden on children living in slums Research shows that child mortality in low-income urban neighborhoods can equal or exceed that in rural areas(4). In Nairobi, Kenya(5) the under-5 mortality rate in slums (151 per 1000 live births) was 2.5 times higher than the average of the city. There is diversity between the slums themselves, with child mortality rates of 254 and 123 per 1000 live births in two different Nairobi slums. This has been seen in other intra-urban studies. In areas with inadequate services (of water supply, sanitation, good health care), morbidity and mortality rates can vary with a factor of 10 -20 or more than better-equipped slum areas of the same city(6). Surveys in seven slum settlements in Karachi found that infant mortality rates varied from 33 to 209 per 1000 live births(6). Table I summarizes findings of three different studies within slums, signifying that in addition to differences within low and high-income areas of a city, the health burden on children within low-income areas also varies. TABLE I Differential Impact on Child Health within Low Income Neighborhoods in an Urban Area.
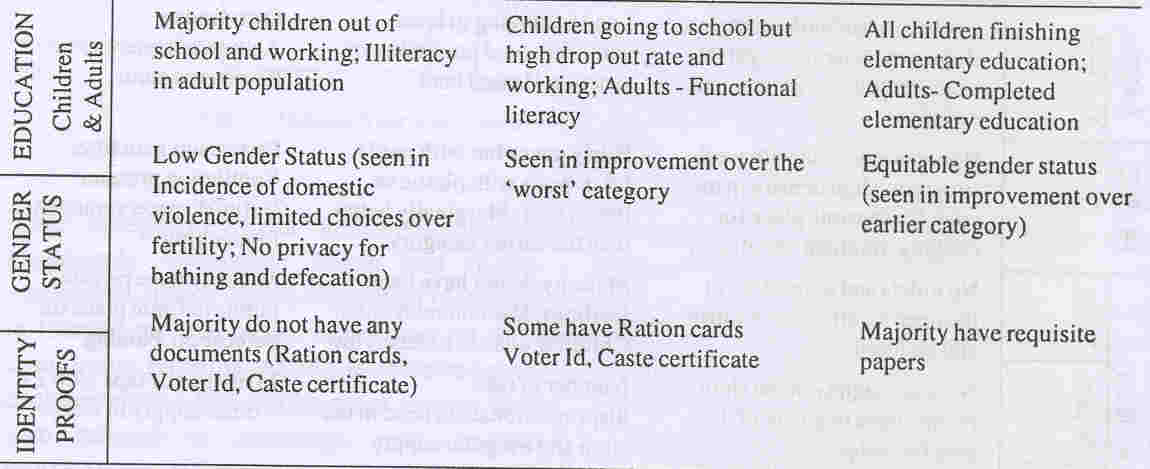
Variable situations in slums affecting child health Studies show associations of various factors and children’s health. Where some argued that reducing income inequalities will be effective in reducing childhood morbidity and mortality(10), there is growing evidence that non-income factors also play a significant role in lowering IMR(11). While traditional practices are associated with poor child health in some slum areas, this is not true in many slum areas where communities can identify biomedical conceptualization of disease processes(12). This section outlines factors impacting child health conditions in urban poor settlements, and thereby needing focus in programs aiming at better child health. (a) Location of impoverished settlements Slums are usually settled on land not used by others for any regular purposes(13). These could be low-lying lands, areas near railway lines or drains, riverbanks or peri-urban areas. Each of these has its own peculiar depreciating factors. Slums located adjacent to large open drains have a greater incidence of diarrhea and other water-borne diseases(14). Slums adjacent to waste disposal sites face several hazards of degraded environment as polluted water and air (personal observation). Pigs, vultures and other animals affect the levels of hygiene maintainable in a slum and thereby increase the risk of spread of infection amongst children who come in close contact with the outside environment (personal observations during slum visits). Slums are almost always initially informal settlements with no land tenure rights. In most cities this "illegal status" of slums and hence the constant threat of eviction continues for years to decades. This result in a sense of resignation among slum dwellers about their surroundings and well being and compromised motivation to invest in infra-structure (required for ensuring children’s health). (b) Unrecognized slums Hidden and missing pockets of urban poverty such as limestone and brick-kiln workers, construction site workers, workers of local industry (leather, jute, glass) are clusters where services usually do not reach, as they are not part of official slum lists. Bound to a specific industry, they are usually on some private land, unseen by most. Owing to long delays in updating of official slums list in most cities, slums may remain unrecognized for years. Evidence from detailed assessment of slums in Dehradun(15), Indore(16) and Bally(17), shows that the proportion of unlisted slums to listed slums is significantly high (a) in Dehradun, 28 unlisted slums were identified beyond the official 78 (35.89%); (b) 159 unlisted slums exist in Indore beyond official list of 438 (36.3%) and (c) in Bally 47 unlisted slums against 75 listed ones (62%). (c) History of interventions Slums that have had program inputs usually have greater awareness on health and other issues. The same slums reap the benefits of different programs year after year owing to (a) slums lists not being updated regularly, (b) greater political awareness and negotiation capacity among relatively better-off slums. "The people whose needs justify the whole development industry are the people with the least power to influence development and to whom there is least accountability in terms of what is funded and who gets funded"(18). (d) Poor water and sanitation Child mortality and morbidity (diarrhea in particular) have been associated with poor water quantity and quality, lack of sanitation and poor hygiene practices. Conditions differ with some slums having adequate water points, while people of other slums having to stand in queues to access poor quality water. Similarly, there are slums without any access to sanitation services. Some are lucky enough to have public latrines (which could be ill maintained)(19). In certain slums, access to health services is fairly good (nearby health facility or Anganwadi center), but open defecation and ineffective drainage system leads to higher incidence of childhood diarrhea. In pediatric practice this background information about a patient’s family can help the pediatrician counsel more effectively and regularly regarding diarrhea prevention. (e) Access to health services: Availability and quality Health facilities proximal to slums affect awareness and health behaviors. A study conducted in Bangladesh(20) showed that children living in communities where outreach clinics were farther than 2 miles were 30 percent less likely to be immunized than children living in communities where outreach clinics were within 2 miles. A survey conducted in the slums of Indore provide evidence that access to essential services such as delivery and immunization is different across different categories of slums: complete immunization was 34, 45 and 49 per cent for the most vulnerable, moderately vulnerable and others slums, while the percentage of home deliveries were 69, 50 and 38 for those slums respectively(21). Within a slum, households close to the main street have greater access to the Auxiliary Nurse Midwife or other health workers as compared to the houses deeper in the slum where paths are muddy and difficult to reach (personal observation in slums). This scenario contributes to well-intentioned programs often not reaching all slum dwellers. ICDS, which covers a population of approximately 28 million(22), has a poor reach in urban areas, with only 278 urban ICDS projects out of 4348 projects(23). Presence of an Anganwadi centre in a slum has been positively associated with decreased malnutrition amongst children and a lower Infant Mortality Rate(24). In Agra, with a slum population of approximately 9,00,000 across 513 slums, there are only 95 Aangan Wadi Centers (AWCs) leaving large slum clusters outside ICDS coverage(24). ( f ) Employment patterns A study(25) in urban centers of Tamil Nadu, showed that households relying on daily earnings cook once a day with a daily purchase of around 100 g of fresh vegetables. Households that relied on weekly earnings were able to better plan food expenditure and save by buying some items in bulk. Slum pockets with uncertain daily wage employment are more vulnerable to health and nutritional deficits. (g) Literacy levels Emphasis on education creates avenues for gaining information, capabilities, confidence and eagerness to try alternative approaches of earning. Slum pockets characterized by low education and literacy levels are hence more vulnerable to poor child health. For instance, a pocket of 70 Pardhi tribal families engaged in rag-picking are labeled ‘dirty’ and ‘unwanted’ by others. Children from this (and other similar slum clusters) are unable to get integrated into nearby schools, owing to poor social acceptance (personal observations in slums in Bhopal, Madhya Pradesh). Studies also show that children and adolescents who work as garbage pickers in refuse dumps have higher school dropout rates(26). (h) Traditional customs In several communities, women (who are primary care givers) remain cut off from health information and continue to follow unhealthy practices affecting children’s health. For example, in slum communities’ home deliveries (often by unskilled persons) and neglect of childhood immunization is often the norm. Pediatricians in independent private practice or working in Hospitals/Health centers will need to persuasively counsel families from such communities regularly for timely immunization and other heath services. (i) Gender status The status of mothers in the families affects children’s health and survival. A study in Nicaragua urban and rural households, found that the risk of death in infancy or before 5 years was two-fold with any history of violence to the mother from her partner and six-fold if she had experienced both physical and sexual violence from her partner(27). There is growing recognition that gender equity positively affects the women’s and her children’s health by enhancing her ability to acquire and use information and take decisions. A study in slums of Karachi(28) reveals a two to three times higher risk of child mortality in households where husbands or other family members were involved in decision-making compared to households where the child’s mother was the main decision-maker. This is probably due to delay in seeking appropriate health care when maternal autonomy is sidelined. Assessing differential health vulnerability across slums The above discussion clearly brings out the need to understand the differential vulnerability of different slum populations, and develop program strategies to improve child health based on this understanding. But how do we do this? An analysis of past vulnerability assessment studies(29-31) shows that poverty and vulnerability assessments have been conducted with the family as a unit. A vital principle for child health programs is that health should be seen as an issue of larger settlements and not as individual or household level problems. This can be better understood through the following points: (a) Caring and health is not affected by household level factors alone. It is a cumulative impact of social customs, living conditions, family conditions and access to services. (b) In an urban health program, input in terms of service delivery, demand generation and behavior promotion, environmental improvements, or building community’s linkage with providers, are workable at the community or cluster levels, not at household levels (c) When improvements occur, collective synergy of the community in terms of social capital and common resources play a vital role. The pride that the community evinces say, on cleaning up the slum, or putting an efficient drainage system in place, is also shared by the community as a whole. This spirit of collective social action and pride is fundamental to human development, and encourages communities to think about, contribute to and soon carve the course to the well-being of their children. Approach Environmental Health Project, a reproductive and child health improvement program of USAID/India focusing on urban areas, has carried out several city based slum identifying and assessment exercises. Figure I depicts the process adopted. Data was collected from slums against the developed criteria by teams of trained people. A ranking key (Table II), assessment criteria for differential vulnerability was developed denoting the levels of conditions within each criterion. A score of 0-2 was given to each criterion, with a score of 0 on the criteria denoting vulnerable condition, and a maxi-mum score of 2 showing a fairly better off condition. The total scores were distributed in three categories: Less vulnerable slums, moderately vulnerable slums and highly vulnerable slums. Slums were thus classified in these three categories depending on their cumulative score based on the assessment on each criterion. The results were triangulated and refined in meetings with various stakeholders to arrive at verified, largely accurate information.
Table II Assessment Criteria for Differential Vulnerability
Outcomes of slum assessment exercise The slum identification and assessment exercise has helped in locating slums and classifying all slums based on their health vulnerability. Studies in two cities show that the proportion of vulnerable slums among unlisted category is significantly higher than that among the listed slums: (a) Dehradun (population 4,50,000), 14 of the 78 officially listed slums were highly vulnerable while corresponding number for unlisted slums was 12 in located 28(15); (b) Bally, West Bengal (population 2,70,000) 27 of registered 75 slums and 23 of 48 unregistered slums were assessed to be highly vulnerable(17). Empirical validation of differential child health care in slums Results for the baseline survey in Indore provide quantitative evidence that the above approach of assessing differing vulnerability of slums is fairly accurate and can help program target resources more effectively. Table III presents the results of the baseline survey(21) carried out in the slums of Indore. TABLE III Results of the Baseline Survey of the Slums of Indore.
The test of significance (t-test) was applied for the key variables by area. The difference was found significant for almost all the above indicators. Limitations of the slum vulnerability assessment exercise • The Assessment Exercise provides an understanding of the city’s slums in a particular period. However, it is important to bear in the mind that, slum scenarios constantly change, owing to seasonal migrations, relocations of slums, shifting of construction sites etc. • Population estimates of slums are crude, as they are based on estimations from group discussions and transect walks. The way forward Many program evaluations and assess-ments(36) have recognized that while meeting measurable success in terms of coverage data, the programs have not succeeded in reaching the most disadvantaged. A study(37) of the ICDS program in seven cities of India concluded that ‘Coming to the population within the slums selected for the study, it was found that even there, the services were not reaching all the poor within the slum, some of the people were excluded for a variety of reasons, ranging from concentration of certain ethnic groups to mixed patterns of residence, non-availability of accommodation, unsuitable timings etc.’ The general impression was that the neediest groups seemed to be the ones left out. The following directions will help reach the neediest in a more responsive way. (a) Identification, assessment and mapping of all slums in a city, is most important for (a) Prioritizing the most needy child health vulnerable slums; (b) identifying hitherto unlisted slum pockets; (c) planning specific need based implementations. This will help address inequity and exclusion. Public health impact of limited resources will also be maximized. (b) Based on assessment, different child health programs can better respond to differential requirements of different slum clusters in a city; for example: Scenario I: When diarrhea is the major morbidity in a group of slums, strategies should focus on three important aspects: (a) improved water availability through augmented supply or by encouraging adequate storage at household level, (b) sanitation improvement through community toilets or individual household toilets, depending on the prevailing context and (c) Hygiene behavior promotion (especially hand washing at critical junctures(38) and safe disposal of feces especially children’s feces(35). Scenario II: If in a group of slums, low immunization coverage of children is the major issue, program efforts should focus on (a) increasing information among slum dwellers about working hours of the Urban Health Center and vaccination schedule in case people are motivated but they lack information regarding services available, (b) conducting immunization camps in needy slums (where physical access and motivation are poor) as well as mobilizing the community to utilize camps services, (c) using context appropriate behavior change communication approaches in slums, where traditional beliefs against vaccination exist.
In Dehradun, the Government’s Urban Health Plan has (a) prioritized more frequent (fortnightly) outreach camps for vulnerable slums, (b) proposed to encourage families from less vulnerable slums to access Urban Health Center for services. In the past, the Government Health Programs used to conduct outreach camps only in registered slums; the new approach will help health services to become more responsive to the differential needs irrespective of the legal status of slums. (c) It is crucial to ensure that the poorest and the neediest are included. In the most child health vulnerable slums, the community by virtue of having low social capital (in the form of collective confidence and abilities) would take longer time to be adequately receptive to program efforts. Providers would also require greater persuasion to strengthen service delivery to such disadvantaged slums, since these are difficult to work in. Evaluation of the Water-Aid Bangladesh Urban Health Program has shown that, planning and management systems must be organized in a way that both respect the limited time that the poorest people have for any personal business and acknowledge their inherent shortage of endowments: "a very poor household may be able to afford one pot of water for drinking purposes but not be able to pay for water for cooking, bathing and laundry’(32). Keeping these issues in mind, an urban slum childhood program should build context-appropriate approaches for encouraging the community as well as the provider to achieve improved health of children. Pediatricians, Clinicians and other personnel engaged in Urban Health Programs should recognize and respond to the social and financial disadvantages of slum dwelling communities by following more effective measures to improve the child health condition in urban slums. Acknowledgement This research was supported by the USAID through the Environmental Health Project managed by Camp Dresser Mckee International Inc. The authors are grateful to Dr. Massee Bateman, USAID and Sarah Fry, EHP, Washington for reviewing the manuscript and providing insightful comments at various stages. Research support and encouragement provided by Pradeep Patra and Madhvi Mathur is acknowledged. The authors are deeply indebted to stakeholders including slum dwellers in various cities that helped learn several aspects of health vulnerability of slums described in the paper.
| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
References | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
![]()