|
|
Original Articles Indian Pediatrics 1999; 36:249-256 |
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
WIDESPREAD OUTBREAKS OF MEASLES IN RURAL UTTAR PRADESH, INDIA, 1996: HIGH RISK AREAS AND GROUPS |
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
From the National Institute of Communicable Diseases, 22 Shamnath Marg, Delhi 110 054, India; *Ministry of Health and Family Welfare, Nirman Bhawan, New Delhi 110 011, India and +National institute of Communicable Diseases, B 20/44 Bhelupura, Varanasi 221010, India.
Measles vaccination was introduced in lndia under the Universal Immunization Programme (UIP) during I 985-86( I). The overall reported coverage increased to 87% in 1994-95(2). Consequently, the measles incidence declined from a reported J 60,216 cases in 1985 to 61,381 cases in 1994(2). However, there had been wide variations in measles vaccine coverage between different states and also among different districts of a state. As a result, outbreaks of measles are still reported from many areas, especially tribal and remote regions(1). These outbreaks should be seen as excellent opportunities to analyze why they occurred, identify high risk areas or groups and measure vaccine efficacy(3); the information generated is useful for their further prevention and control Keepjng this in view, we present here an account of a large outbreak of measles which affected many districts in Uttar Pradesh (UP) during 1996. Methods With a population of more than 139 million (l991census), Uttar Pradesh is the most populous state in India. Population density is 473 per sq km, and 85% of the population live in rural areas. Crude birth and death rates are 35.4 (national 28.6) and 11 (national 9.2) per 1000 population (1994 SRS provisional data), respectively(4). The state has very high mortality rates (1993 SRS); IMR 93 per 1000 live births and child mortality rate of 32.9 per 1000 under 5 children against a national figure of 74 and 23.7, respectively(5). The authors reviewed the state data on measles morbidity, mortality and vaccine coverage from 1991 through 1996. Data for the earlier years were: not readily available. However; line lists on measles cases for the year 1996 were available for some of the districts at the Directorate of Family Welfare, Uttar Pradesh, Lucknow. These were analyzed to ascertain the age, immunization status, geographical distribution, and age and sexspecific fatality of measles during the present outbreak. A house to house survey was organized in 7 measles affected villages of a Primary Health Center (PHC) in Lucknow district during 8-9 July 1996 to estimate vaccine efficacy. The PHC had reported 40 measles cases (median age <5 years) by first week of July in 1996; 1 case in March, 35 cases in June and 4 cases in July. Using a standard questionnaire, paramedics interviewed parents. (mostly mother) of under 5 children to collect data about their children' age, sex, history of measles' since 1 JanuaryJ996, and immunization status against measles before illness. The standard clinical casedefinition(6) was used for the mothers to recall the episodes of measles amongst their children. Only a few 'children had immunization cards~ Children were therefore, labelled immunized or not immunized according to records available with the health personnel or from convincing histories of immunization given by the mothers. A large number of children had been vaccinated against measles recently in response to the outbreak. These vaccinations were not taken into account for calculation of vaccine efficacy. Vaccine efficacy was calculated for children above 9 months of age using the basic formula of vaccine efficacy: VE=(ARUARV)*100/ARU; where ARU=attack rates in unvaccinated, ARV=attack rates in vaccinated. Finally, we reviewed the results of coverage surveys carried out in UP from 1992 through 1996(7 -9) to find out the gaps between the reported and estimated measles vaccine coverage. Chi-square test was. used to test the difference between proportions. A p value of <0.05 was considered significant. . Results Fifty one of 68 districts in UP reported 6922 cases and 281 deaths due to measles in 1996. Overall case fatality ratio (CFR) was 4.1 %. Majority of the deaths occurred in Badaun, Gorakhpur, Siddarthnagar, Basti, Maharajganj, Bareilly, Lakhimpur Kheri, Sitapur, Moradabad and Faizabad districts. There was heavy clustering of cases and deaths in rural areas; only endemic pattern was observed in urban communities.
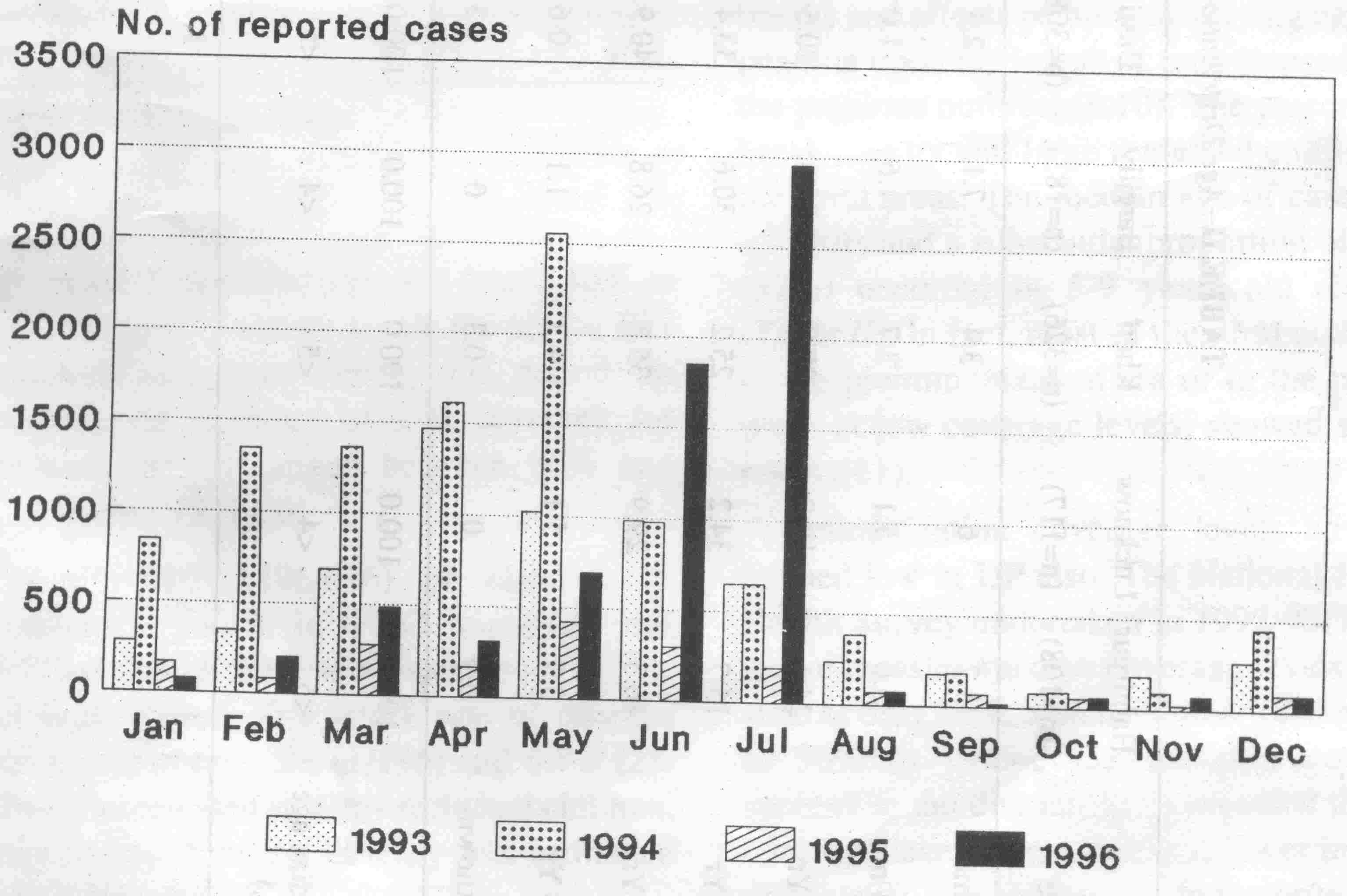
The reported incidence of measles in the state from 1992 to 1996 is shown in Table I. The disease is endemic in UP. The incidence showed a rise on alternate years. As illustrated in Fig. 1,the majority of cases (and deaths) in 1996 occurred in June and July which are low. transmission months in northern India. TABLE I
TABLE II
TABLE III
Table IV describes the vaccination status of measles cases in 7 districts for which data were available. About 85% of the cases denied history of measles vaccination. Virtually, all deaths occurred in unimmunized children. TABLE IV Immunization Status of Measles Cases *
Examination of data from statewide coverage surveys undertaken during 1992-96 revealed a very poor measles immunization coverage in UP(7-9). Only 26% of the children received measles vaccine by I year of age in 1992; the coverage was found .36% in 1996. In fact, coverage levels for all the EPI vaccines were poor during this period. In contrast, the reported official coverage for measles vaccine ranged between 88% and 93% during 1991-96! Only 32% (196/616) of children (9 months-<5 years) in PHC surveyed had received a dose of measles vaccine before the outbreak started. The attack rate of measles was found to be 0.5% (1/196) and 6.7% (28/ 420) in vaccinated and unvaccinated children, respectively. Vaccine efficacy was estimated to be 92%. Discussion The present outbreak of measles in UP showed a pattern which is consistent with the transmission dynamics of measles. Dense urban areas with huge population (at moderate or even at high coverage levels) can sustain measles transmission throughout the year resulting in most of the infections by 3 years of age. In contrast, in predominantly rural communities, measles occurs in sporadic outbreaks and affects persons of varying ages depending upon the length of time elapsed since the previous outbreak(6, to). The present outbreak also by and large remained confined to the rural areas. The median age of cases was <5 years and a substantial proportion of cases (37%) occurred in 5-9 years old children (Table II). In fact, most of the rural outbreaks in the pre immunization era or in the present times at low coverage levels, showed similar results(11). Immunization coverage levels have remained low in UP also. The National Family Health Survey undertaken in 1992-93(7) estimated measles vaccine coverage levels in the state as only 26%, which increased marginally to 36% in 1995-96(8). Separate coverage surveys in the districts have revealed that the coverage levels are even much lower in many districts(9). Occurrence of the majority of the cases in unvaccinated children (85%) during the present outbreak is also indicative of very poor coverage levels for measles vaccine (Table IV). Conversely, routine reporting system showed that very high coverage levels (>85%) have been achieved in the state. A clear gap was therefore, evident between reported coverage and survey results. In fact, Chandra and Mohan have recently shown that large gaps existed in virtually all the districts in Uttar Pradesh due to poor performance and over reporting(9). They suggested (i) delinking immunization from the incentive based programmes monitored at district levels; (ii) improving immunization supplies and transport facilities; (iii) in-service training of health workers; and (iv) special campaigns to improve the coverage in problem villages. Incidentally, a clear tendency has been observed that lower the real coverage, the greater the difference between the reported coverage and survey results(l2-14). These issues need to be addressed if the goals of universal immunization, measles control, neonatal tetanus elimination and poliomyelitis eradication are to become a reality in Uttar Pradesh. The outbreak provided an excellent opportunity to measure vaccine efficacy. Community surveys revealed a vaccine efficacy of 92% which indicates that vaccine failure was not probably a major factor in the present outbreak. An excellent surveillance is essential for early detection and expert investigation of cases, compilation and analysis of data that will influence policies, identification of high risk areas and groups, and monitoring of efficiency and progress(3). However, the surveillance for measles was found to be very poor in Uttar Pradesh. Less than 1 % of the estimated measles cases in the state [even after accounting for 36% vaccine coverage(8) and 40% subclinical measles infections(15)] were found to be reported through routine surveillance system, and estimated measles deaths were many times the reported cases (authors' estimate, data not shown). What to speak of more complex analysis, even month wise, district wise measles cases and deaths in the last few years were not readily available with the state EPI unit. It is thus obvious that there is an urgent need to strengthen the routine surveillance system in the state, otherwise the goal of measles control may not be within our reach despite a tremendous decline in the measles incidence in India(1). The age-specific CFR was found to be the highest (6%) in under five children (Table Ill) and thereafter declined with increasing age. These results are consistent with an earlier review on measles mortality in India(16), and highlight the importance of immunization at the earliest recommended age to prevent measles mortality in younger children. . Overall, females had significantly higher CFRs than males (6.3 vs 3.8%). Sex: differences in measles mortality were found at all ages; however, excess female mortality between ages 5 to 9 years was more pronounced and statistically significant (Table Ill). An earlier documented outbreak(17) and a 13 year long prospective study in rural Ur(8) also showed higher CFRs from measles in females than males. The mechanisms underlying the observed sex differences in the CFRs are not fully understood. Preferential treatment of sons and concomitant daughter neglect which are common in the predominantly rural population of UP(19) may be blamed by someone for excess female mortality from measles. Nevertheless, excess female mortality from measles had also been observed in rural Senegal without having an apparent. difference in parental attitude towards boys and girls, especially in respect to health maintenance(20). Based on a review showing an excess female mortality from measles at age 0-50 in all the major regions of the world, Garenne recently suggested that biological differences between sexes rather than behavioral factors may be responsible for excess female mortality from measles(21). A plausible explanation for sex differences in the CFRs probably lie in two recent observations: (i) Female infants experienced much higher mortality than male infants following vaccination with high titer measles vaccine(22); and (ii), adult females exhibited a strong humoral immune response to the standard titer measles vaccipe(23). It may be postulated that the excess female mortality from measles result from a strong. immune response to the measles infection, accompanied by a greater general immunosuppression effect during the period following acute measles infection. Nevertheless, strong negative beliefs about measles and nonavailability of quality health care may partly explain an overall high CPR in rural India, especially during the outbreaks. Being a traditional rural community having low literacy rates, people in Uttar Pradesh usually do not seek timely treatment for postmeasles complications like diarrhea and pneumonia which are primarily responsible for high fatality in measles( 17). An overall CFR of 4.1% was reported in the state during the present outbreak (Table /). However, rural Lucknow being more literate and having better health care due' to its proximity to the, state capital did not record any measles deaths, whereas Badaun, a backward district having relatively poor health care services, recorded a CFR of 23%. Finally, the outbreak occurred largely in unvaccinated population. Although, availability of timely and appropriate health care including administration of vitamin A is crucial in preventing mortality, a very high coverage with measles vaccine may also lower mortality from measles(24). Unless we increase the coverage levels rapidly, such widespread outbreaks will continue to occur in states like UP. Thus, there is an urgent need to achieve and sustain high vaccine coverage levels in all districts and communities to control measles as a major step towards its global elimination in the longer run. Acknowledgements The authors acknowledge the cooperation of following health professionals from the Directorate of Health & Family welfare, Uttar Pradesh for carrying out this study: Dr. R.K. Dubey, Director of Family Welfare; Dr. Anurag, Joint Director (EPI); Dr. A.C. Srivastava, Research Officer; Dr. Amrendra Singh, Chief Medical Officer (CMO); Dr. A.B. Sinha and Dr. P.K. Tiwari, Deputy CMOs; and Dr. Rajeev' Banswal, , Senior 'Medical Officer.
| ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
![]()