|
|
|
Indian Pediatr 2017;54: 512-513 |
 |
Congenital Junctional Ectopic Tachycardia in
a Neonate
|
|
*Mani Ram Krishna and Usha Nandhini Sennaiyan
RK Hospital for Women and Children, Thanjavur.
Email: [email protected]
|
|
Congenital Junctional ectopic tachycardia (JET) is a rare and usually
incessant tachyarrhythmia that presents in the first few months of life.
In the past, treatment of congenital JET was difficult, and the
condition was associated with a high mortality [1]. However, with the
evolution of amiodarone as the first line of pharmacological management,
the outlook for infants with this disorder has improved [2]. We report a
neonate with congenital JET who had an incessant arrhythmia, and was
managed on a combination of amiadarone and propranolol.
A late pre-term (34 weeks 6 days) baby was delivered
via emergency cesarean section. A routine antenatal scan had
documented a heart rate of 210/minute and fetal ascites. The liquor
volume was normal. Clinical examination of the infant showed a pulse
rate of 210/min with good peripheral pulses and normal peripheral
perfusion. The respiratory system examination, cardiac examination and
abdomen were normal. Echocardiogram revealed a structurally normal heart
except for a persistent small atrial communication shunting left to
right. The ventricular contractility was preserved on subjective
assessment.
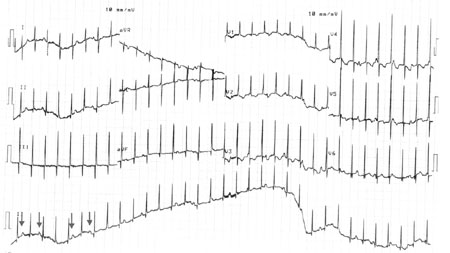
The electrocardiogram (ECG) showed a narrow complex
regular tachycardia with a heart rate of 200/minute (Fig. 1).
There was evidence of atrio-ventricular (A-V) disassociation with an
atrial rate of 150/minute. A diagnosis of congenital JET was made and
the baby was started on propranolol at a dose of 1 mg/kg/dose four times
a day. There was no suppression of tachycardia in 48 hours although the
baby remained hemodynamically stable. Hence amiodarone was added at a
dose of 10 mg/kg/day followed by a maintenance dose of 5 mg/kg/day.
After 4 days of treatment, a satisfactory rate control with reduction of
the junctional rate to approximately 120/minute was achieved and the
child was discharged on the combination of amiodarone and propranolol.
 |
|
Fig. 1 ECG showing a regular
narrow complex tachycardia with a heart rate of 200/minute and
evidence of A-V dissociation. The arrows denote p waves which do
not have a consistent relationship with the QRS complexes.
|
Congenital JET is a rare neonatal arrhythmia that was
first reported by Coumel, et al. [3]. It is caused by abnormal
automaticity of the A-V node. The ECG typically manifests as a
narrow-complex tachycardia with evidence of A-V disassociation or 1:1
retrograde V-A condition. JET with onset in the first few weeks of life
is more likely to be incessant or sustained (>50% of QRS complexes) with
a high risk of congestive cardiac failure [1,2,4]. Most children require
a combination of anti-arrhythmic medications, with amiodarone the most
commonly used [2]. Complete or partial control of arrhythmia is possible
in only about one-third of cases.
References
1. Villain E, Vetter V, García JM, Herre J, Cifarelli
A, Garson A. Evolving concepts in the management of congenital
junctional ectopic tachycardia. A multicenter study. Circulation.
1990;81:1544-9.
2. Collins KK, Van Hare GF, Kertesz NJ, Law IH,
Bar-Cohen Y, Dubin AM, et al. Pediatric nonpost-operative
junctional ectopic tachycardia: medical management and interventional
therapies. J Amer Coll Cardiol. 2009;53:690-7.
3. Coumel P, Fidelle JE, Attuel P, Brechenmacher C,
Batisse A, Bretagne J, et al. [Congenital bundle-of-his focal
tachycardias. Cooperative study of 7 cases]. Arch Mal Coeur Vaiss.
1976;69:899-909.
4. Sarubbi B, Musto B, Ducceschi V, Cavallaro C,
Vecchione F, Musto C, et al. Congenital junctional ectopic
tachycardia in children and adolescents: a 20 year experience based
study. Heart. 2002;88:188-90.
|
|
|
 |
|
