|
|
|
Indian Pediatr 2017;54:
503-504 |
 |
Right Atrial Diverticulosis and Early-onset
Arrhythmia: Rare Cause of Incessant Neonatal Arrhythmia
|
|
Neeraj Aggarwal, *Raja
Joshi, *Reena K Joshi and Mridul Agarwal
From Department of Pediatric Cardiology and
*Pediatric Cardiac Sciences, Sir Ganga Ram Hospital, New Delhi, India.
Correspondence to: Dr Neeraj Aggarwal, Consultant
Pediatric Cardiology, Sir Ganga Ram Hospital, Rajender Nagar, New Delhi
110 060, India.
Email: [email protected]
Received: June 16, 2016;
Initial review: October 14, 2016;
Accepted: March 29, 2017.
|
Background: Atrial flutter not responding to medications could be
secondary to structural malformations of heart. Case characteristics:
A 5-year-old child with resistant arrhythmia, with onset in neonatal
period. Outcome: Multiple right atrial diverticuli were detected
on CT angiography and cardiac catheterization. Patient reverted to sinus
rhythm following surgical excision of diverticuli. Message: In
cases of intractable supraventricular tachycardia, structural anomalies
of atrium should be suspected.
Keywords: Atrial Diverticulosis, Neonatal arrhythmia,
Palpitation.
|
|
R
ight atrial diverticulum (RAD) is a rare
structural abnormality with varied presentations from incidental
cardiomegaly on chest X-ray/echocardiography to incessant
arrhythmias. We present a child presenting with atrial flutter from
neonatal age that was eventually diagnosed as due to right atrial
diverticulosis, and was successfully treated by surgical resection of
the diverticuli.
Case Report
A 5-year-old boy presented to our facility as an
out-patient with recurrent palpitations. Examination revealed a
well-oriented, anxious looking child with a regular heart rate of
210/min and a blood pressure of 95/45(52) mm Hg. Electrocardiogram (ECG)
showed typical saw tooth appearance suggestive of atrial flutter with
fast ventricular rate. Past history revealed that he has been having
such episodes dating back from the neonatal period. The first episode of
supraventricular tachycardia was documented at 4 hours after birth. It
was reverted with intravenous adenosine. Thereafter, there have been
many similar episodes necessitating multiple visits to the emergency and
outdoor departments of the local area. He had received various
anti-arrhythmic medications for paroxysmal, intractable flutter with
limited control. Trans-thoracic echo reported previously was normal.
During the present episode, there was no response to
adenosine, therefore cardio version was planned. Preparatory to
cardio-version, Trans-esophageal echo (TEE) was performed to rule out
intracardiac thrombus. TEE revealed an abnormal septation in the right
atrium (RA) communicating freely with the cavity without any
intracardiac clots. At this point of time, differential diagnosis of cor
triatriatum dexter, RA aneurysm or RA diverticulum was entertained. CT
angiogram showed finger like projections originating from RA suggesting
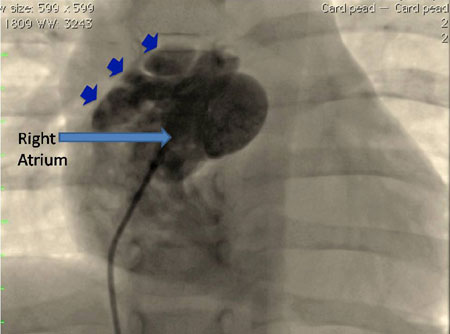
the possibility of RA diverticuli. Cardiac catheterization was done with
contrast injection showing multiple out-pouching from RA free wall
suggestive of diverticulosis of RA (Fig. 1). After an
informed consent from the parents, child was taken up for surgery.
Prophylactic amiodarone was started in the operating room.
Intra-operatively multiple diverticuli were seen in the right atrial
free wall and appendage. Diverticuli were excised including RA appendage
and surgical ablation of arrhythmogenic focus was performed. The rhythm
reverted to sinus immediately after resection and stayed sinus
thereafter. Child had uneventful postoperative period and got discharged
on 4th post-operative day. Oral amiodarone was prescribed at the time of
discharge which was weaned off over the next 6 weeks. After 18 months
follow up, child is asymptomatic, and has a normal 24-hour Holter
evaluation.
 |
|
Fig.1 Catheterization image showing
multiple out pouches (small arrows) from right atrium suggestive
of diverticuli.
|
Discussion
RA diverticulum is a rare anatomical abnormality and
neonatal presentation of multiple RA diverticuli has not been described
often. The etiology of these diverticuli is not clearly understood.
There is a single case report of familial occurrence, although genetic
preponderance is not established [1]. Shah, et al. [2]
reported a neonate presenting with SVT and
Wolff-Parkinson-White syndrome associated with a single RA diverticulum
where the patient was managed medically [2]. Neonatal SVT is usually
associated with a structurally normal heart. Incessant supraventricular
tachycardia has been found to be associated with some of the structural
malformations; the commonest being Ebstein’s anomaly followed by
cortriatriatum dexter, congenital enlargement or aneurysm of right
atrium and diverticuli of atria. These malformations present as
cardiomegaly and atrial enlargement. Echocardiography usually can
differentiate these anomalies, although in some instances further
radiological investigation like MRI, CT angio, or cardiac angiography
are required.
Binder, et al. [3]
reviewed 103 cases of congenital malformations of
RA and coronary sinus including four cases of multiple RA diverticuli,
with three of these presenting with SVT. Minimum age at presentation of
these patients was 5 months [3]. RA diverticuli causes SVT either by
providing surface area for circus movements (Atrial re-entrant
tachycardias) or by directly stimulating the cardiac surface (Ectopic
atrial tachycardia). Surgical excision of diverticuli removes the
substrate and cures the SVT. Patients usually do not have recurrence of
arrhythmias after surgery.
It has been suggested that surgery should be offered
to symptomatic patients and asymptomatic patients should be managed
conservatively [3]. However, others feel that as there is a high risk of
thrombus formation, arrhythmia and rupture of diverticuli in these
patients, and also considering low operative mortality, asymptomatic
patients should also be offered surgical treatment [4]. This is
especially more true for diverticuli of coronary sinus and multiple
diverticuli of RA who have high incidence of arrhythmias compared to RA
aneurysm.
In cases of intractable SVT in neonates and infants,
structural anomalies of atrium should be suspected and adequately
evaluated with echocardiography and other radiologic modalities.
Therapeutic outcomes are good in cases of RA diverticulum.
Contributors: NA: data acquisition and clinical
study was performed; NA, RJ: manuscript preparation, editing, review and
literature search; RKJ, MA: concept and design of study was done; NA,
RJ: guarantor and take full responsibility and confirm the originality
of the work performed. The manuscript has been read and approved by all
the authors.
Funding: None stated. Competing interest:
None stated.
References
1. Jenni R, Goebel N, Schneider L, Krayenbuhl HP.
Familiae idiopatihe dilatation des rechten vorhofs. Schweiz Med
Wochenschr. 1981;111:1565-72.
2. Shah K, Walsh K. Giant right atrial diverticulum:
an unusual cause of Wolff–Parkinson–White syndrome. Br Heart J.
1992;17:874-82.
3. Binder TM, Rosenhek R, Frank H, Gwechenberger M,
Maurer G, Baumgartner H. Congenital malformations of the right atrium
and the coronary sinus. Chest. 2000; 117:1740-8.
4. Agematsu K, Okamura T, Ishihara K and Kurosawa H.
Remarkable giant right atrial diverticulum in asymptomatic patient.
Interact Cardiovasc Thorac Surg. 2009;8:705-7.
|
|
|
 |
|
