| |
|
Correspondence Indian Pediatrics 2008; 45:513-514 |
|||
|
Hypernatremic Dehydration Leading to Peripheral Gangrene |
|||
|
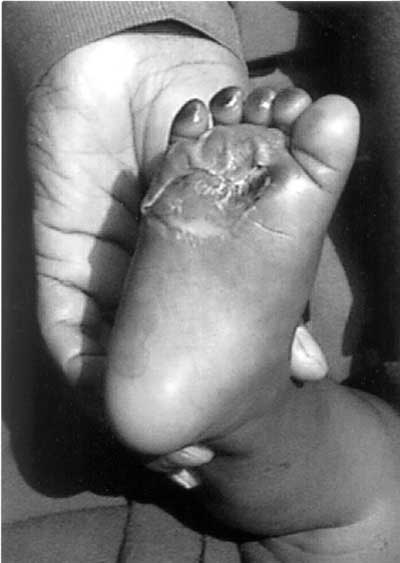
We report a 8 month old infant who presented with loose watery stools 30-40/day, vomiting 6-8/day and excessive crying for 3 days. The infant had received home made sugar salt solution, intravenous fluids and injections before coming to our hospital. There was no history of cannulation in the lower limbs. The child did not have any convulsions. On examination the child was irritable and moderately dehydrated. The toes of both the feet were gangrenous, the parents had noticed discolouration of toes 1 day prior to admission (Fig 1). The anterior fontanel was level and the peripheral pulses were palpable. There was no hypertonia and the deep tendon reflexes were brisk with no neurological deficit. Initial investigation revealed blood urea of 107.4 mg/dL, serum creatinine of 1.1 mg/dL and serum sodium (Na+) and potassium (K+) were163 meq/L and 2.2 meq/L, respectively. The platelet count was 60,000/mm3, prothrombin time was 20 seconds (control 13) and activated partial thromboplastin time was 50 seconds (control 38). The blood sugar, serum calcium and cerebrospinal fluid examination were normal. Treatment was instituted for hypernatremic dehydration along with antibiotics and supportive care. The Na+ and K+ levels gradually returned to 144 meq/L and 3.4 meq/L on third day, and to 140 meq/L and 4.4 meq/L on day 5, respectively. The platelet count was 2.4 lacs/mm3 on day 5 of admission. The kidney function also returned to normal. The child improved clinically and gangrenous feet started healing.
Hypernatremic dehydration is not very commonly seen because thirst is a very effective mechanism in preventing hypernatremia. It usually occurs if there is limited access to water or because of inappropriate preparation of ORS or home made rehydration solution. It is usually seen in extremes of age or in a sick or debilitated patient. In this type of dehydration there is shift of water from intracellular to extracellular compartment and therefore signs of extracellular depletion are masked. These patients are lethargic and very irritable with hypertonia and hyperreflexia(1). Peripheral gangrene secondary to hypernatremic dehydration is very rare although it has been reported earlier(2-4). Hypernatremic dehydration may lead to gangrene because of hypoperfusion and hyperviscosity which leads to sluggish blood flow and disturbed micro-circulation(4). In most cases, it is associated with disseminated intravascular coagulation(5). DK Singh,
|
![]()