|
|
Case Reports Indian Pediatrics 2007;44:438-440 |
||
|
Splenic Abscess as a Complication of Enteric Fever |
||
|
Rajoo Thapa
From the Department of Pediatrics, The Institute of Child Health, Kolkata, India. Correspondence to: Dr. Subroto Chakrabartty, BF–212,
Sector I, Salt Lake City, Kolkata 700 064, Manuscript received: August 1, 2006; Initial review
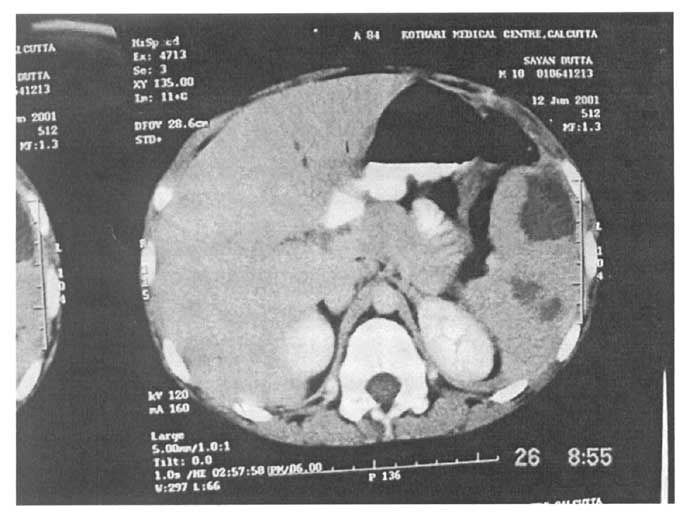
completed: September 29, 2006; Enteric fever, Splenic abscess. Splenic abscess is a rare complication of typhoid fever. About 34 cases are described since 1977, most of them solitary but a few had multiple abscesses. The clinical diagnosis of splenic abscess due to typhoid fever is difficult because of its rarity, insidious onset and nonspecific clinical presentation(1,2). It is often fatal if left untreated. Case Reports Case 1 A 10-year-old male child presented with a 15 days history of fever and abdominal pain. The patient was febrile (102.4ºF) and had generalized abdominal tenderness, more so in the left upper quadrant with minimal muscular guarding. Laboratory tests demonstrated: hemoglobin 11.0 g/dL; white blood cells count of 4800/mm3 (52% neutrophils, 44% lymphocytes), platelet count 320,000/mm3. Serum urea, creatinine levels and urinary analysis were normal. Blood culture was positive for Salmonella typhi. Widal test was also positive (T: O at 1: 320 dilution). Urine and stool cultures for the same organism were negative. The child was started on Ceftriaxone and Ofloxacin. However, despite antibiotic therapy, fever, abdomi-nal pain and abdominal tenderness persisted. Abdominal ultrasound (US) revealed multiple hypoechoic areas in the spleen; the largest being 42 mm in diameter. Computed tomography (CT) findings (Fig.1) corroborated with the diagnosis of multiple splenic abscesses. Sickling test and HIV screen were negative. Splenectomy was performed since multiple splenic abscesses were inappropriate for percutaneous drainage.
Case 2 A ten-year-old male child presented with high grade, remittent fever for the last one-month and pain abdomen for last 7 days. On examination, the boy had a toxic look, was irritable and febrile (103ºF). He had mild tachypnea and tachycardia. There was diffuse abdominal tenderness, more marked over the left hypochondrium. There was moderate hepatosplenomegaly. Laboratory tests demonstrated : hemoglobin 9.0 g/dL and white blood cells count of 19,200/mm3 (36% neutrophils, 54 % lymphocytes). Serum urea, creatinine levels and urinary analysis were normal. The Widal test was positive at 1 in 160 dilution. Cultures of the blood, urine and stool were sterile. Abdominal ultrasound revealed a space occupying cystic lesion in the spleen measuring 5.5 × 4.9 cm. The child was started on Ceftriaxone and Ofloxacin. Percutaneous splenic aspiration yielded 70 mL of pus. Culture of the pus revealed the growth of S. typhi. After apparent initial improvement, the child was febrile again with pain abdomen on day 8 of admission. Repeat US examination showed a similar cystic lesion in the spleen measuring 4.8 × 4.4 cm. Conservative surgery which included deroofing of the abscess cavity was done. The boy improved subsequently and repeat US at the end of two weeks showed complete resolution of the abscess. Discussion Splenic abscess as a complication of typhoid fever is a distinct rarity. The more common causes of splenic abscess are infection due to Staphy-lococcus species and Bacteriodes(3). Non typhoidal salmonella are more frequently reported than S. typhi. Factors leading to the development of splenic abscess are usually impaired host resistance, subacute bacterial endocarditic, trauma, diabetes mellitus, urinary tract infection, skin sepsis, respiratory tract infection and intravenous drug abuse(2). Sickle cell disease is also present in about one-third of patients with splenic abscesses(4). Multiple splenic abscesses are found in immuno-deficient patients (especially HIV positives) who have poor prognosis(1). A few cases with multiple splenic abscesses caused by S. typhi are described in the literature. Allal, et al.(2) reported 400 patients with S. typhi and found splenic abscess in 8 (2%) cases; of these only one had multiple splenic abscess. Torres, et al.(5) documented 10 cases of typhoidal solitary splenic abscesses. In splenic abscess, CT evaluation is more specific than US evaluation in delineating gas bubbles, which is diagnostic for splenic abscess, in visualizing the peripheral contrast enhancement and in providing clear demonstration of the location of the abscesses(2). MRI may reveal some clues in the diagnosis by defining the extent and internal structure of splenic abscess because of its greater tissue resolution(6). Until recently, the treatment of splenic abscesses was splenectomy with antibiotic therapy. The recent trends are more conservative because the immunologic role of the spleen has been better understood over the last years(7). Solitary unilocular abscesses may respond well to percutaneous drainage. Multiple or loculated abscesses may respond to antibiotics alone(8) but splenectomy is the preferred treatment(1). In general, failure to respond to antibiotics with or without percutaneous drainage necessitates splenectomy(8). In conclusion, splenic abscess should be considered as a complication of enteric fever when fever and toxicity does not abate with adequate antimicrobial therapy, especially when the child has localizing clinical features i.e., left hypochondrial pain, scoliosis etc. Non-invasive imaging modalities including US, CT and MRI are useful for early diagnosis of splenic abscess. Contributors: RT–manuscript drafting and review; KM–data acquisition and compilation and SC–overall coordination and guidance. Funding: None. Competing interests: None stated.
| ||
|
References | ||
|
|
![]()