|
The assessment of renal size is
an integral part of
evaluation of renal diseases for both diagnostic
and prognostic purposes. Sonography is a non-invasive modality for measuring renal size. Data on normal renal size
are available from western population [1-3]. Indian data
regarding renal size and its correlation with other somatic parameters
in normal Indian children are based on studies with a small sample size
and sparse age distribution [4-9]. The present study was undertaken to
determine renal size in normal Indian children (1 month-12 years).
Methods
Normal children aged 1 month and 12 years were
eligible for inclusion in the study. The children were either healthy
siblings of patients attending the out-patient clinics or those visiting
well-baby clinics. Consent was obtained from the accompanying parents.
Children suffering from any acute or chronic ailment were excluded from
the study. Age, weight and height were recorded at the time of the
examination. Infants were weighed on an infant weighing scale and older
children on a beam balance. Weights were recorded to the nearest 100 gms.
The supine lengths were measured on an infantometer in children below 2
years and the standing height was measured on a stadiometer in children
above 2 years to the nearest 1 mm. One investigator took all the
measurements. The body surface area (BSA) was calculated from weight
[10].
A Philips real-time mechanical sector scanner of
3.5-5 MHZ frequency with electronic calipers was used to measure the
length, width and thickness of each kidney with the child placed in a
supine oblique position. The maximal renal length was recorded after
re-positioning the probe in several angulations. Renal width was
measured at renal hilum and thickness was recorded from transverse scans
showing the maximum dimension. All the measurements were made by one
investigator. The mean of right and left kidney measurements was used in
all calculations. The renal volume was calculated by the formula
[1]:Volume = 0.5233 × length × width × breadth.
The mean length, width and volume ±2 SD of the right
and left kidneys were calculated separately for age groups of 1 month, 3
months, 6 months, 9 months, 1 year, and every year thereafter throughout
12 years. Length and volume were the two (dependant) variables of renal
size considered for correlating with somatic parameters. Regression
equations and coefficients of correlation were derived for each pair of
variables. The statistical difference among the groups was determined by
t test. Coefficient of correlation was derived by Pearson coefficient of
correlation. Statistical analysis was performed using SPSS software.
Results
There were 1000 children (480 females) in 16 age
groups from 1 month to 12 years of age. The number of children within
each age group ranged from 35 to 120 with a mean of 77 children. The
mean renal length (SD) increased steadily with age from 4.3 (0.6) cm at
1 month to 8.6 (0.8) cm at 12 years of age. The mean renal volume (SD)
increased from 9.7 (4.4) mL at 1 month to 61 (17) mL at 12 years (Table
I).
TABLE I Mean Renal Length and Volume of Study Children (N=1000)
| Age |
Weight (kg) |
Height (cm) |
Body
surface |
Renal
length (cm) |
Renal
volume (mL)
|
|
Mean
(SD) |
Mean
(SD) |
area
(m2) (SD) |
Mean
(SD) |
Mean
(SD) |
| 1 mo
(n=71) |
2.5 (0.4) |
48.5 (2.1) |
0.18 (0.02) |
4.3 (0.6) |
9.7 (4.7) |
| 3 mo
(n=49) |
3.7 (0.9) |
53.8 (4.2) |
0.23 (0.05) |
4.7 (0.7)
|
12.1 (6.0) |
| 6 mo
(n=61) |
5.6 (1.1) |
61.8 (4.4) |
0.32 (0.05) |
5.5 (0.7) |
18.3 (7.0) |
| 9 mo
(n=81) |
7.3 (0.9) |
68.5 (3.7) |
0.39 (0.03) |
5.6 (0.6)
|
19.6 (6.8) |
| 1 y
(n=122) |
8.5 (1.1) |
72.0 (2.8) |
0.44 (0.04) |
5.7
(0.4)
|
21.3 (5.5) |
| 2 y
(n=75) |
9.7 (1.4) |
79.0 (7.6) |
0.48 (0.05) |
6.1 (0.7)
|
25.3 (8.2) |
| 3 y
(n=58) |
11.2 (1.5) |
89.2 (5.0) |
0.54 (0.05) |
6.7
(0.6)
|
31.3 (10.0) |
| 4 y
(n=63) |
12.9 (1.0) |
95.7 (4.2) |
0.59 (0.03) |
6.8 (0.60)
|
32.9 (9.1) |
| 5 y
(n=66) |
14.0 (1.7) |
101.1 (4.3) |
0.62 (0.05) |
6.7 (0.6)
|
33.0 (8.9) |
| 6 y (n=54) |
16.5 (2.2) |
107.5 (5.2) |
0.69 (0.06) |
6.7 ( 0.4)
|
34.2 (9.4) |
| 7 y (n=48) |
18.0 (2.1) |
112.5 (5.5) |
0.74 (0.06) |
7.2 (0.6)
|
44.6 (12.7) |
| 8 y (n=57) |
20.6 (2.2) |
116.8 (6.0) |
0.81 (0.05) |
7.6 (0.7)
|
49.8 (14.8) |
| 9 y (n=58) |
24.0 (2.7) |
125.8 (4.1) |
0.88 (0.06) |
8.0 ( 0.6)
|
56.2 (16.7) |
| 10 y (n=43) |
25.9 (3.9) |
130.4 (5.8) |
0.92 (0.08) |
8.0 (0.7) |
58.0 (16.2) |
| 11 y (n=32) |
30.9 (4.3) |
138.9 (5.3) |
1.02 (0.09) |
8.5 (0.8)
|
59.8 (17.3) |
| 12 y (n=62) |
31.9 (4.5) |
141.7 (5.8) |
1.04 (0.09) |
8.6 (0.8)
|
61.4
(16.5) |
|
*SD: standard deviation; mo= months; y=year. |
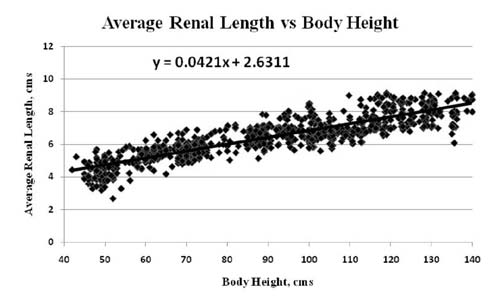
There was a good correlation of renal size with age,
body weight, body height and BSA The best correlation was of renal
length with the body height (r=0.9) and body surface area (r=0.89).
Renal volume also had good correlation with body height in cms (r=0.85).
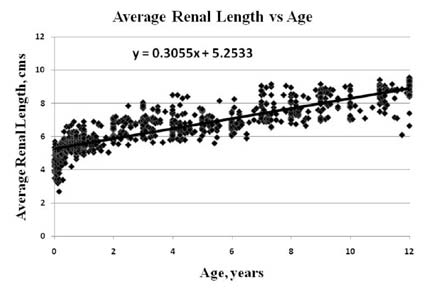
Fig.1 shows scatter diagrams of mean renal length with
body height and age, respectively. Linear regression equations for
predicting variable (renal length) from independent variables (age and
height) were obtained as follows: Renal Length = 0.0421 × height +
2.6311; and Renal Length = 0.3055 × age + 5.2533.
 |
 |
|
Fig. 1 Regression equation of (i) renal
length vs body height (ii) renal length vs age.
|
Discussion
In the present study the renal size correlated well
with most commonly used parameters of overall body size including age,
body weight, body height and body surface area. The best correlation of
renal size was seen with body length and body surface area. While the
renal volume correlated best with body surface area.
Although body proportion and rate of general somatic
growth are strikingly different between boys and girls, their renal
lengths did not display a significant difference. Other studies have
also reported similar observations [1, 3, 9-11]. A number of studies
have assessed renal size and volume in children and have correlated to
somatic parameters. As with our findings with respect to correlation,
other studies have revealed similar results [6-11]. In children with
growth failure and under-nourished children, it will be better to
correlate the renal length with the body length [14]. Judged by
sonography, the renal length in Indian children was lower by 11-20% as
compared to American children with respect to age, probably due to the
larger body size of their American counterparts [2]. Had we compared
with body height, the difference may have been less. Comparison of renal
volume and BSA of Indian children with those of American children may
have shown less difference.
There are numerous advantages of ultrasonography in
determining renal size. They include the lack of ionizing radiation
exposure, radiographic magnification and osmotic effect of the iodinated
contrast material [2]. The examination is real time, tridimensional,
independent of organ function and phase of respiration. Previously the
kidney size was accurately measured on intra venous urography which had
its own disadvantages [15-17]. Although the renal length correlated best
with body height and body surface area, the calculation of body surface
area is cumbersome and requires multiple measurements. In clinical
practice, the body height can be quickly recorded to compare the actual
renal length with the renal norm. Similarly, since the estimation of
renal volume requires measurement of three dimensions of the kidney, the
error associated with renal volume increases in geometric proportion.
Hence it is simpler to use renal length as a yardstick for comparing
renal growth with body growth. Due to the large sample size, this study
represents the population more closely. However, the
socioeconomic status of children examined was not recorded, although
they typically belonged to lower middle and lower income group.
Considering the large population of India, the study did not consider
parameters such as race, culture, income group, rural or urban origin.
The renal size norms developed by this study provide
normal kidney length range for children according to age and body size.
Acknowledgments: Mr Abhiram Behera
(Biostatistician), for conducting the statistical analysis.
Contributors: KM and UA conceived the study and
revised the manuscript for important intellectual content. UA and AO
were involved indata collection, interpretation and analysis, and
drafting the article. MN conducted the sonographic evaluation and
revised the manuscript.
Funding: None; Competing interests: None
stated.
|
What is Already Known?
•
Sonography-based renal size in
Western population groups.
What This Study Adds?
•
Sonography-based renal size in normal Indian children aged 1
month-12 years and linear regression equation to predict renal
size from length/height of children.
|
References
1. Han BK, Babcock DS. Sonographic measurements and
appearance of normal kidneys in children. AJR Am J Roentgenol.
1985;145:611-6.
2. Rosenbaum DM, Korngold E, Teele RL. Sonographic
assessment of renal length in normal children. Am J Radiol.
1984;142:467-9.
3. Haugstvedt S, Lundberg J. Kidney size in normal
children measured by sonography. Scand J Urol Nephrol. 1980;14:251-5.
4. Mehta KP, Karnik SR, Sathe A, Pant R, Khatwan R,
Bhise A. Renal parameters during infancy. Indian Pediatr.
1992;29:1385-90.
5. Gupta AK, Anand MK, Lamba IS. Ultrasound
evaluation of kidney dimensions in neonates. Indian Pediatr.
1993;30:319-24.
6. Dixit PK, Sahai SB, Rath B, Garg A, Chowdhary V.
Norms for renal parenchymal volume in Indian children. Indian Pediatr.
1994;31:1059-64.
7. Mathur S, Chandra J, Mittal KP, Mittal SK, Khurana
A. Sonographic assessment of renal length in Indian children. Indian J
Pediatr. 1996;63:553-60.
8. Chattopadhyay P, Bhatnagar V, Gupta AK, Mitra DK.
Ultrasonography assessment of renal growth in normal Indian children.
Indian J Urol. 1998;14:22-5.
9. Ganesh R, Vasanthi T, Lalitha J, Rajkumar J,
Muralinath S. Correlation of renal length with somatic variables in
Indian children. Indian J Pediatr. 2010;77:326-8.
10. Vaughan VC III, Iris LF. Growth and development.
In: Behrman, Kliegman, Nelson, Vaughan, editors. Nelson Textbook of
pediatrics. 14th ed. WB Saunders Company Harcourt Brace Jovonovich Inc :
1992. p. 40.
11. Schlesinger AE, Hernandez RJ, Zerin JM, Marks TI,
Kelsch RC. Interobserver and intraobserver variations in sonographic
renal length measurements in children. Am J Radiol. 1991:156:1029-32.
12. Ece A, Gozu A, Bukte Y, Tutanc M, Kocamaz H. The
effect of malnutrition on kidney size in children. Pediatr Nephrol.
2007;22:857-65
13. Currarino G. Roentgenographic estimation of
kidney size in normal individuals with emphasis on children. Am J Radiol.
1965;93:464-6.
14. Ekf O, Ringertz H. Kidney size in children: a
method of assessment. Acta Radiol Diagn (Stockh). 1976;17:617-25.
15. Hodson CJ, Drewe JA, Karn MN, King A. Renal size
in normal children: a radiographic study during life. Arch Dis Child.
1962;37:616-22.
|


