|
|
Research Papers Indian Pediatrics 2008; 45:547-553 |
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
Oral Salbutamol for Symptomatic Relief in Mild Bronchiolitis: A Double Blind Randomized Placebo Controlled Trial |
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
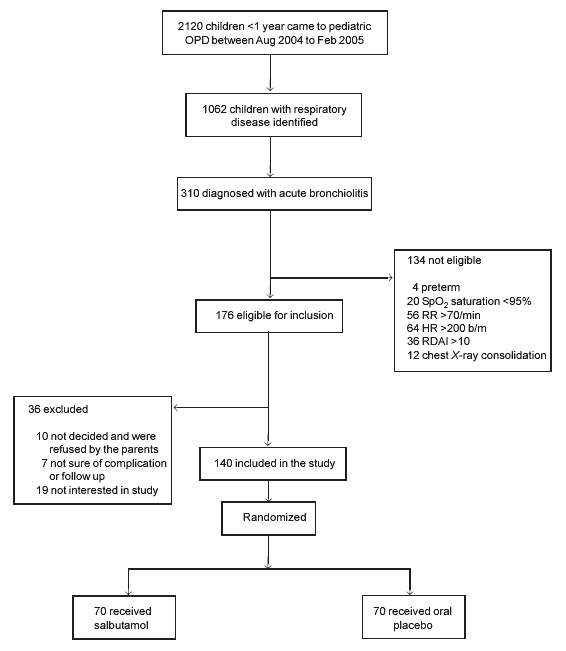
Introduction Bronchiolitis is considered to be a self limiting disease. Majority of cases are of mild severity(1), which can be managed on outpatient basis. Traditionally, the treatment has been supportive. Clinicians, however, desire to have a drug for symptomatic relief of bronchiolitis, which would decrease the physical and mental agony of children and their parents, reduce hospital revisits and retard progression of severity of disease; and decrease the admission rate. Data about the efficacy of bronchodilators in the management of bronchiolitis beyond the emergency department visits are inadequate; and most studies are conducted on nebulized drug delivery(2-14). Only a single study till date by Patel, et al.(3), has evaluated the role of oral salbutamol administration in mild to moderate bronchiolitis. We planned this double blind, randomized, placebo controlled trial to assess whether oral salbutamol brings about a faster symptomatic relief in children with mild bronchiolitis. Methods This study was a double blind, randomized, placebo controlled trial, conducted at the Pediatric outpatient department (OPD) of a tertiary care hospital in North India. The study population consisted of consecutive infants below one year of age, clinically diagnosed with acute bronchiolitis. Bronchiolitis was defined as first episode of wheezing with evidence of an acute viral respiratory tract infection (coryza, axillary temperature >38oC, cough, predominant wheeze/rhonchi on chest auscultation and suggestive radiograph). Infants were included only if they had a mild disease characterized by respiratory rate £70 breath/min, heart rate £200 beats/min, hemoglobin oxygen saturation (SpO2) ³95% in room air, no or mild accessory muscle use, and respiratory distress assessment instrument (RDAI) score £10. Children were excluded if they were dehydrated, lethargic, had an underlying chronic cardiopulmonary disease, or had history of administration of bronchodilators in this episode. Protocol of the study was fully explained to the parents/guardians of study participants and an informed consent was obtained. Clearance from the ethical committee of the institution was obtained. Participants were randomized in two groups using urn method. All study personnel and participants were blinded to treatment assignment for the duration of the study. Both study syrups looked and tasted alike. Numerically coded opaque brown bottles were prepared for dispensing the drugs, containing similar amount of the drug. The study drug was administered orally by a pre-marked and labeled container. Children were assigned to receive either oral salbutamol (0.1 mg/kg/dose) or placebo, three times daily for a maximum of 7 days or until the symptoms resolved. The first dose was given in the OPD, and the method of administration was taught to the caregiver. Any patient who vomited the drug within 15 minutes of ingestion was advised to have a repeat dose. All caregivers were asked to maintain a record of consumption of doses and doses missed, in a small diary. Parents in both the groups were advised a standard care protocol that included humidification of environment, steam inhalation, continuation of feeds, plenty of fluids, and antipyretic administra-tion. Paracetamol (15mg/kg/dose) was the only other drug co-administered with the study drug and was used only on SOS basis. Parents were also counseled about the danger signs (increasing retraction, noisy breathing, lethargy, refusal of feeds, alteration in sensorium, blueness of body) and asked to report them immediately. Children who developed danger signs were admitted and provided therapy as for severe bronchiolitis. Children were followed up on day 3, 7, and 14 after enrolment. At each follow up visit, parents were asked regarding the resolution of illness, presence and severity of bronchiolitis symptoms including cough, fever and coryza, feeding and sleeping pattern of the infant along with overall health status of the infant and adherence with the prescribed therapy. Adverse events like tremor and vomiting were also recorded. Parents of those infants who did not report for follow-up were contacted telephonically and asked for the resolution of illness or deterioration of the clinical status. Baseline data recorded include age, sex, birth weight and gestation (if known), and the present weight. Details of breastfeeding, duration of present illness, symptoms at presentation and the RDAI score were recorded. Cardiorespiratory status was assessed by recording respiratory rate, heart rate, and hemoglobin oxygen saturation (SpO2) at room temperature. Respiratory distress was quantified by using the Respiratory Distress Assessment Instrument (RDAI), a 17 point categorical score developed by Lowell, et al.(15). The primary outcome variable was time to resolution of illness (ROI)(3). This was defined as the time from study enrollment to the time the infant returned to baseline health status, as determined by principal caregiver. A 4-point scale was used for scoring the ROI. Parents were asked to score their infant’s symptoms as follows: 1-worsening of symptoms, 2-same symptoms, 3-lessening of symptoms, and 4-resolution of symptoms. The time to achieve score of 4, i.e., the time to resolution of symptoms was compared between the two groups. Duration of cough, cold, noisy breathing, time to resume normal feeding and time to resume normal sleeping served as the secondary outcome variables. The two groups were also compared in terms of revisit and hospital admission rates. Sample size and statistical analysis: A minimum of 70 children in each group was required to detect a mean difference of 2 days in resolution of illness, with a standard deviation of 4 days in each group, type 1a error =0.05 and statistical power of 90%(3). The primary analysis was performed according to intention to treat. Kaplan Meir survival log rank test was employed to analyze the difference in time to ROI between the two groups. Similar technique was used to analyze all secondary outcome measures. Other qualitative and quantitative measures between the two groups were compared by using Chi square and Student’s t-test respectively. Results Subject enrollment is depicted in the study flow chart (Fig. 1). The two groups were comparable in terms of baseline personal characteristics, duration of illness, and cardiorespiratory status (Table I). All children presented with cough, coryza and fever. Fast breathing was present in 56/70 (80%) children in each group. Inadequate oral intake was complained by 30/70 (42.9%) mothers in the Salbutamol group as compared to 28/70 (40%) in the Placebo group (P=0.86). TABLE I Baseline Parameters in the Salbutamol versus Placebo Group
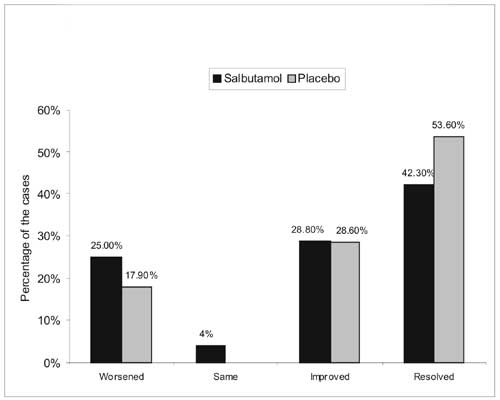
On day 3, 46/70 children reported for follow up in Salbutamol group as compared to 50/70 children in Placebo group. Another 12 children (6 in each group) could be contacted telephonically. Their mothers stated that these children had shown complete resolution of illness and therefore they did not think that it was necessary to come up for the follow up visit. Another 32 children (Salbutamol, 18; Placebo, 14), neither reported on day 3 nor could be contacted telephonically; 24 of these children, however re-entered the study on day 7 for their second follow up visit. Thus on day 3, data were available for 52/70 (74.3%) in the Salbutamol group and 56/70 (80%) in Placebo group. 1 child in each group was lost to follow up at 7 days. Hence a total of 7 children in salbutamol group and 3 in placebo group were lost to follow up. Fig. 2 depicts a qualitative comparison in resolution of illness for these 108 children on day 3, between the two groups. The respiratory rate declined by 12 breaths/minute (from 46 to 34) in the Salbutamol group as compared to 11 breaths/min (from 44 to 33) in placebo group (P >0.05).
By day 7, complete resolution occurred in 57 (81.4%) children in the Salbutamol group; 2 (2.9%) needed admission for worsening of symptoms and another 4 (5.7%) demonstrated partial resolution. These 4 children were followed up at 14 days and mothers reported complete resolution in all of them. In the Placebo group, complete resolution occurred in 65/67 children for whom follow up was finally available; 2 children needed hospitalization. A total of 10 subjects were lost to follow up, 7 (10%) in the Salbutamol group and 3 (4.3%) in the Placebo group.
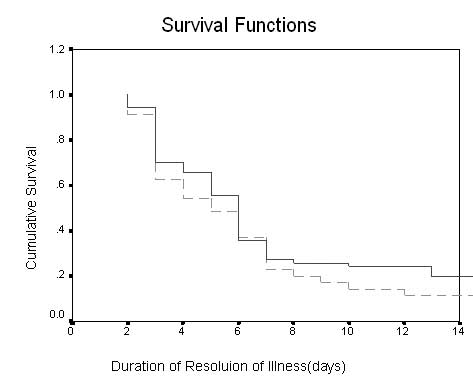
Median ROI (SE, 95% CI) as assessed by survival analysis was 6 (0.5 to 7) days in the Salbutamol group as compared to 5 (1, 4 to 6) days in placebo group (P=0.21) (Fig. 3). Comparison of mean duration for resolution of individual symptoms, between the two groups is shown in Table II. Adverse effects included tremors/trembling in 5 children (all from Salbutamol group), vomiting in 6 (Salbutamol: 2; Placebo: 4), and irritability in a single child in the Placebo group. TABLE II Resolution of Symptoms in Salbutamol and Placebo Group
Discussion We conclude that oral salbutamol is not superior to placebo in providing symptomatic relief in infants with mild bronchiolitis. These results are consistent with the only other randomized controlled trial conducted in Canada by Patel, et al.(3). Though both these studies demonstrated identical results on outcome parameters; yet the duration of resolution of illness (ROI) was longer in the previous study (median 8 days) as compared to our study (median 5 days). This can be attributed to a less severe form of illness in our subjects as shown by the shorter duration of illness (1.5-2 days vs 4 days in previous study). Difference may be attributed to different genetic and ethnical background of the two study populations. Also, the etiological agent in the earlier study(3) was predominantly RSV; while it could be a mixed bag in our study. Gadomoski, et al.(16,17) conducted double-blind placebo controlled studies with oral and nebulized salbutamol in children with bronchiolitis. These studies showed no demonstrable efficacy of salbutamol in relieving respiratory distress. However, the major limitation of these studies was that the follow-up of respiratory rate, heart rate and SpO2 were done at 30 and 60 minutes following oral administration of salbutamol. Orally consumed salbutamol/placebo is unlikely to get absorbed and attain serum levels within 1 hour of consumption. The period of follow-up should have been longer, especially when the drug in question was administered by oral route. Thus, the results of the study were not generalizable, and did not prove or disprove the efficacy of oral salbutamol over placebo in the treatment of bronchiolitis. In our study, follow up was done at 3, 7 and 14 days. The serum level of salbutamol is established by this time to achieve a clinical response. It was observed that the respiratory rate and heart rate declined significantly over time, with no difference with regards to administration of placebo or salbutamol. This indicated and confirmed the self-resolving nature of this viral illness and negated our hypothesis for need of a drug for symptomatic resolution of mild bronchiolitis. Another limitation of Gadomski trials was that the effect of drugs on reducing the overall duration of illness and other symptoms was not analyzed(16,17). Role of b2-agonists in treatment of acute viral bronchiolitis is much more controversial than that of non-selective agents like epinephrine. Salbutamol is the most common drug studied in the treatment of bronchiolitis. Most studies were conducted on nebulized salbutamol(5-10) and very few on oral route(3,16,17). This can be explained by majority of studies being conducted in emergency departments rather than out patient settings, and where giving an oral drug would have raised few ethical and technical problems. Major limitation of our study was that the diagnosis of bronchiolitis was entirely clinical and virological confirmation was not sought. It meant that some cases with non-viral etiology of lower respiratory tract infection would have been included, though this anomaly would be equally existing in both the study and control groups due to simple randomization. Also, significant number of cases did not turn up for follow-up and were contacted telephonically. Results in these cases were entirely based on parent’s perception, without objective evaluation. On the basis of our results, we recommend discontinuation of practice of prescribing oral salbutamol for the symptomatic relief in the cases of mild bronchiolitis. Contributors: The study was conceived by PiG. All authors contributed to study design. Data were collected by PaG under the supervision of AA and PiG; and analysed and interpreted by PiG, AA, PaG and KKS. The article was drafted by PaG and AA. PiG and KKS revised it critically for important intellectual content. The final version was approved by all authors. Funding: None. Competing interests: The drug and placebo were packaged and dispensed at the Pharmacology department of the College without any grant, free supply or sponsorship. The authors do not benefit in any form, from the sale or promotion of the drug used in this study. This study was awarded the ST Achar Gold Medal at PEDICON 2006.
| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
References | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
b2-agonist in bronchiolitis: A reappraisal and meta-analysis. Pediatrics 1997; 100: 233-239. 12. Wang EEL, Milner R, Allen V, Maj N. Bronchodilators for treatment of mild bronchiolitis. A factorial randomized trial. Arch Dis Child 1992; 67: 289-293. 13. Ho L, Collin G, Landau LI, Le Souef PN. Effect of salbutamol on oxygen saturation in bronchiolitis. Arch Dis Child 1991; 66: 1061-1064. 14. Hughes DM, Lesouef PN, Landa u LI. Effect of salbutamol on respiratory mechanisms in bronchiolitis. Pediatr Res 1987; 22: 83-86. 15. Lowell DI, Lister G, Von Koss H, McCarthy P. Wheezing in infants: response to epinephrine. Pediatrics 1987; 79: 939-945. 16. Gadomski AM, Aref GH, El Din OB, El Sawy IH, Khallaf N, Black RE. Oral versus nebulized albuterol in the management of bronchiolitis in Egypt. J Pediatr 1994; 124: 131-138. 17. Gadomski AM, Lichenstein R, Horton L, King J, Keane V, Permutt D. Efficacy of albuterol in the management of bronchiolitis. Pediatrics 1993; 93: 907-912. |
![]()