|
|
Short Communication Indian Pediatrics 2007; 44:519-521 |
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
Fixed-Dose Combination of Lamivudine, Stavudine and Nevirapine in the Treatment of Pediatric HIV-infection: A Preliminary Report |
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
Tripti Pensi From the Department of Pediatrics, R.M.L. Hospital, New Delhi, India. Correspondence to: Dr. Tripti Pensi, Department of
Pediatrics, R.M.L. Hospital, New Delhi, India. Manuscript received: October 11, 2006; Initial
review completed: December 5, 2006;
The use of antiretroviral agents in the form of Fixed Dose Combinations (FDCs) in both adults and children is an important consideration as this promotes better adherence and, in turn, limits the emergence of drug resistance(1). I report the preliminary results of my experience with the fixed drug combination of lamivudine, stavudine, and nevirapine (3TC + d4T + NVP) in the form of oral suspension and dispersible tablets in the treatment of pediatric patients infected with HIV. Subjects and Methods This was an open-label, non-comparative, prospective study in clinical setting. Twenty-one HIV-infected pediatric patients were enrolled in this study. Patients were classified into clinical (N, A, B, & C) and immunological(1-3) categories before starting the study medication(2) Baseline clinical assessment, screening for TB and CD4 count was done in every patient. If TB was present it was treated first for 6 months. CD4 count was done by flow cytometry-FACS Counter. Care was taken to draw blood sample at the same time of the day to avoid diurnal variations that occur in CD4 count. Patients thereafter received FDC of 3TC + d4T + NVP in the form of an oral suspension (Emtri; containing d4T 10 mg, 3TC 40 mg and NVP 70 mg per 5 mL)-Group A; or dispersible tablet (Emtri Junior; containing d4T 10 mg, 3TC 40 mg and NVP 70 mg in each dispersible tablet)-Group B. The lead-in period with nevirapine was arranged with separate formulation for 14 days. The dosage schedule of FDCs is provided in Table I. Follow-up was done every 3 months during which patients were assessed for improvement in symptoms, adverse drug reactions (ADR) and CD4 count. All the patients who were enrolled in the study were included in the final analysis. TABLE I Dosage Schedule of FDCs
Results Table II provides the baseline demographic variables of the 21 pediatric patients. TABLE II Baseline Demographic Variables (n=21)
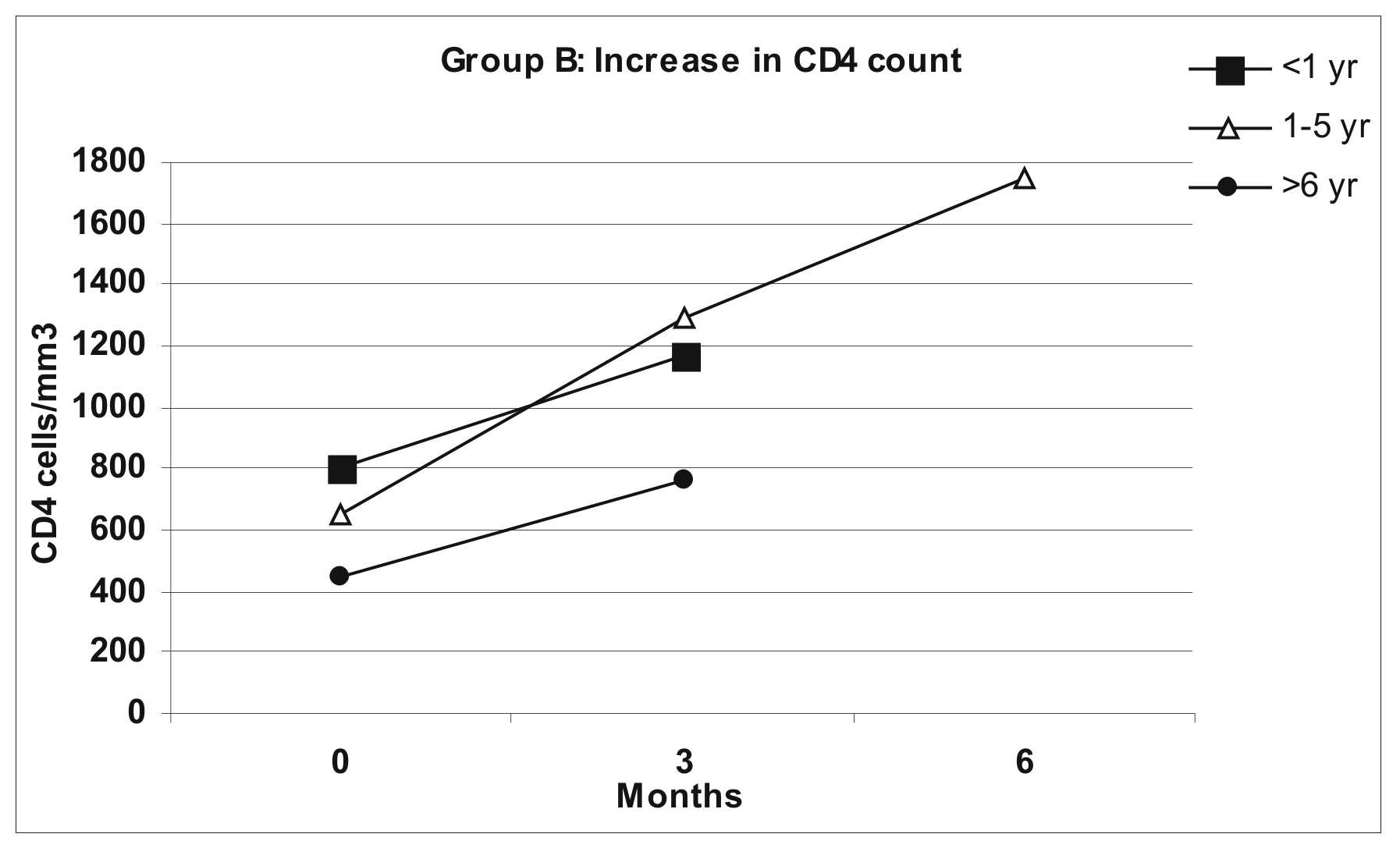
All the patients completed at least 3 months follow-up. The mean increase in CD4 counts in the two groups is depicted in Figs. 1 & 2. At baseline, the number of patients with clinical category B and C in Group A and B were 6, 3 and 7, 5 respectively. At the end of follow-up period, the number of patients with clinical category N and A in Group A and B were 7, 5 and 6, 3 respectively. Improvement in signs and symptoms noted was weight gain, decreased incidence of fever, diarrhea, infections and hospitalization. No adverse drug reaction was observed. Both the FDCs were well tolerated. All the patients in both the groups had SGPT & SGOT values within normal limit at the end of follow-up period. The patient/parent/guardian reported adherence was >95% in all the patients. There were no treatment failures. Discussion An increase in CD4 count of ≥50 cells/mm3 at 4-8 weeks after viral suppression and thereafter an additional 50-100 cells/mm3/year is considered as response to highly active antiretroviral therapy (HAART). The significant improvement in CD4 counts (Figs. 1 & 2) and improvement in clinical status demonstrated in the study confirms the efficacy of medications used.
A study that aimed to describe the effect of HAART in treating HIV-infected children in Thailand’s National Access to Antiretroviral Program for People Living with HIV/AIDS showed that HAART regimen consisting of 3TC+d4T+NVP was safe and effective for HIV-infected children, despite initiation of treatment during the advanced stage of disease(3). Present study showed that the HAART regimen consisting of 3TC+d4T+NVP in the form of pediatric formulations is safe and effective for HIV-infected children in resource limited setting. Poor adherence to HIV medications acts as barrier to treatment in children. Adherence to ART regimen, the extent of at least 95% is optimal(4).Use of FDCs results in simplification of treatment, reduction in the number of pills or volume of liquid to be taken and these factors promote adherence to therapy(5,6). The present study has shown that FDCs were able to achieve high level of adherence in resource poor setting. in addition, they were well tolerated. Thus it is evident that use of such simplified, child-friendly FDCs offer convenience of administration by parents as well as intake by pediatric patients which helps improve adherence to therapy. This, in turn results in improvement in clinical and laboratory parameters indicating disease control. Funding: None. Competing interests: None.
| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
References | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
![]()