|
|
Research Paper Indian Pediatrics 2007; 44:505-510 |
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
Immunogenicity and Safety of Combined Diphtheria-Tetanus-Whole cell Pertussis-Hepatitis B/ Haemophilus Influenzae Type b Vaccine in Indian Infants |
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
S.B. Bavdekar*, P.P. Maiya*, S.D. Subba Rao†, S.K. Datta** and H.L.Bock** From the Seth G.S. Medial College and K.E.M. Hospital, Mumbai, India; *Department of Pediatrics and Neonatology, M.S. Ramaiah Medical College, Bangalore, India; †Department of Pediatrics, St. John's Medical College Hospital, Bangalore, India; **Clinical R&D and Medical Affairs, GlaxoSmithKline Biologicals, Rixensart, Belgium; Vice-President and Director, Clinical R&D and Medical Affairs, GlaxoSmithKline Biologicals, Rixensart, Belgium.Correspondence to: Sanjoy K. Datta, Director Clinical R&D and Medical Affairs - Biologicals South Asia, GlaxoSmithKline Biologicals, Rue de l'Institut 89, 1330 Rixensart, Belgium. E-mail: [email protected] Manuscript received: September 26, 2006; Initial
review completed: November 27, 2006;
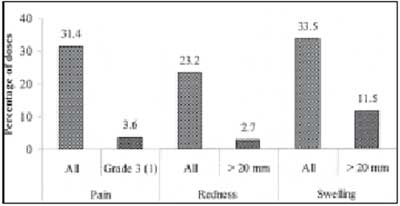
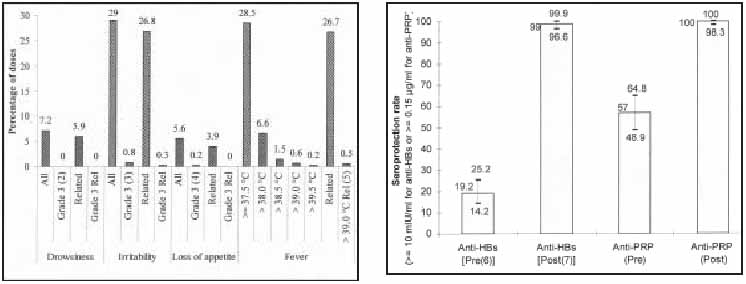
Acombination vaccine including diphtheria, tetanus, Bordetella pertussis (BPT), hepatitis B and conjugated Hemophilus influenzae type b antigens (DTPw-HBV/Hib), which allows the administration of fewer injections, was developed in the 1990s. This vaccine is registered and marketed in more than 80 countries and is pre-qualified by the WHO. This combination vaccine was introduced into global immunization schedules in the 1990s and into India in 2000. Combined immunization against diphtheria, tetanus and pertussis has become routine practice over the past 50 years. Enhanced combination vaccines including hepatitis B and Hemophilus influenzae type b (Hib) antigens were developed more recently(1). These newer combination vaccines have the advantages of reducing discomfort for infants and therefore increasing the rates of acceptance and compliance with vaccine recommendations. Such benefits reduce the logistical costs of vaccine delivery, and ease the introduction of new pediatric vaccines into the already crowded childhood vaccination schedules(2-4). This Phase IV study investigated the immune response to the DTPw-HBV/Hib combination vaccine against the hepatitis B and Hemophilus influenzae type b components and evaluated its safety and reactogenicity when administered to Indian infants according to the local schedule. Subjects and Methods This was an open, phase IV, single group study conducted in three centers across India (one center in Mumbai and two centers in Bangalore) from October 2003 to February 2004. Healthy infants aged six to eight weeks of age and fulfilling inclusion and exclusion criteria were enrolled in the study only after obtaining voluntary written informed consent from the parents or guardians. The subjects were required to have had a dose of hepatitis B vaccine at birth and no significant medical or family history contraindicating vaccination. Subjects who were HBsAg seropositive at the time of vaccination were excluded from the study in addition to subjects who were administered agents which may affect the immune system (e.g., immunosuppressants) or given other vaccines during the study period (with the sole exception of oral polio vaccine). The study protocol was approved by the Drugs Controller General of India (to facilitate subsequent approval for the shipment of sera for analysis by the Director General of Foreign Trade) and all institutional ethics review committees. The study was conducted within the guidelines of the International Conference on Harmonisation’s Good Clinical Practice (ICH-GCP)(5) and subject to an audit by the sponsor (GlaxoSmithKline Biologicals) with no critical findings. Vaccines Commercial lots of the DTPw-HBV and Hib vaccines, manufactured by GlaxoSmithKline Bio-logicals (Rixensart, Belgium), were used in this study. One dose (0.5 mL) of the combined DTPw-HBV vaccine (Tritanrix-HB™) contained ≥30 IU diphtheria toxoid, 60 IU tetanus toxoid, 4 IU whole cell B. pertussis (killed), 10 µg hepatitis B surface antigen, 0.63 mg aluminium salts, 25 µg thiomersal and 500 µg 2-phenoxyethanol and the Hib vaccine (Hiberix™) contained 10 µg conjugate Hib capsular polysaccharide (PRP) conjugated with 20 to 40 µg tetanus toxoid, and 12.6 mg lactose.The DTPw-HBV vaccine was supplied as a liquid vaccine in a monodose vial, while the Hib vaccine was supplied as a white freeze-dried pellet in a monodose vial. The vaccines were reconstituted by dissolving the lyophilized Hib vaccine pellet in the liquid DTPw-HBV vaccine before use, and administered intramuscularly into the anterolateral aspect of the infant’s thigh. Three doses of the DTPw-HBV/Hib vaccine were administered to each infant at 6, 10 and 14 weeks of age, as per the most widely practised local immunization schedule. Reactogenicity analysis All infants were followed up for one month after the final dose. Solicited symptoms occurring during the 4-day follow-up period after each dose were recorded prospectively on diary cards by the parents/guardians and reported to the investigator at the subsequent visit. Local solicited symptoms included pain, redness and swelling at the injection site. General solicited symptoms such as fever [the highest temperature (axillary/oral) recorded daily], irritability, drowsiness and loss of appetite were also recorded by the parents. Unsolicited symptoms occurring during the 30-day follow-up period were recorded retrospectively by the investigator. Serious adverse events (SAE) were monitored during the entire study period. Serological analyses Blood samples were collected prior to the first dose of study vaccine and one month after the third vaccination. Serum samples were stored at –20ºC until sent to the laboratories for testing. Anti- HBs antibody concentrations were measured locally at Thyrocare Technologies Ltd., Mumbai, using automated chemiluminescence immunoassay (IMMULITE, DPC, USA). Concentrations were expressed in mIU/mL. HBsAg at pre-vaccination time point was measured by Radioimmunoassay (AxSYM, Abbott). Anti-PRP antibody concentrations were measured by ELISA using an in-house assay at GSK Biologicals and expressed in µg/mL. Statistical analyses The overall incidence (following all doses) of each local and general solicited symptom reported during the 4-day follow-up period was calculated. Unsolicited symptoms reported during the 30-day follow-up period were tabulated and their relationship to vaccination assessed by the investigator. The percentage of subjects with anti-PRP antibody concentration ≥0.15 µg/mL and ³1.0 µg/mL and seropositivity (≥3 mIU/mL) and seroprotective levels ( ≥10 mIU/mL) of anti-HBs antibody concentration were determined. Geometric mean concentrations (GMC) of antibodies against PRP and hepatitis B vaccine antigens were calculated with 95% confidence intervals (CI).Results A total of 225 subjects (52% males) with a mean age of 6.3 ± 0.5 weeks were enrolled in the study. Six subjects withdrew from the study [one subject due to the HIV-positive parent, two subjects due to migration from the study area, two subjects who were lost to follow-up and one subject due to an SAE (aspiration pneumonia) which was not considered by the investigator to have any causal relationship to vaccination]. A total of 213 subjects were included in the immunogenicity analyses. Twelve subjects were eliminated from the immunogenicty analysis: five subjects due to protocol violation linked to inclusion, exclusion and elimination criteria and seven subjects due to non-compliance with the protocol-defined vaccination and blood-sampling schedules. A total of 670 doses were administered and 663 symptom sheets were completed. Swelling at the injection site was the most frequently reported local reaction [reported following 222 (33.5%) doses] and irritability [reported following 192 (29.0%) doses] was the most frequently reported general symptom. Redness ≥20 mm and swelling >20 mm were reported after 18 (2.7%) and 76 (11.5%) doses, respectively; severe pain (cried when limb was moved/spontaneously painful) was reported following 24 (3.6%) doses (Fig. 1 and Table I). Fever exceeding 39.5ºC was recorded following only one dose in one subject. The percentage of doses followed by severe solicited general symptoms (symptoms that prevented normal activity) and severe unsolicited symptoms did not exceed 0.8% (Fig.2 and Table I) and 0.4% respectively. Two SAEs were reported (acute gastroenteritis with dehydration and death following aspiration pneumonia); neither was considered to be related to vaccination by the investigators.
One month after the third vaccination, all subjects had seroprotective levels of anti-PRP antibodies (concentrations ≥0.15 µg/mL), 98.6% had anti-PRP antibody concentrations ≥1 µg/mL and the GMC was 22.824 µg/mL. The anti-HBs seroprotection rate (percentage of subjects with anti-HBs antibody concentration 10 mIU/mL) was 99% and the GMC was 408.2 mIU/mL (Fig. 3 and Table II).Table I Incidence of Solicited Local and General Symptoms Reported during the 4-day Follow-up Period after Vaccination
N: number of documented doses; n (%): number (percentage) of doses followed by the symptom; Grade 3 pain: Cried when limb was moved/ spontaneously painful; Grade 3 drowsiness: Drowsiness that prevented normal activity; Grade 3 irritability: Crying that could not be comforted/ prevented normal activity; Grade 3 loss of appetite: Not eating at all; Related: symptoms considered by the investigator to be causally related to vaccination; LL, UL: Lower and upper limits of 95% confidence interval. Discussion This study was specifically undertaken not only to determine the reactogenicity of the vaccine but also to enhance the available immunogenicity data of the HB and Hib components of the vaccine. The study included infants who had been vaccinated with HBV at birth, as recommended by the IAP and WHO(6). Since India has moderate endemicity of hepatitis B infection and carriage and as pregnant women are not routinely teted for hepatitis B surface antigen, a birth dose would prevent almost 100% of vertical transmission of hepatitis B to newborns. This has also been seen in other countries where a high proportion of chronic infections is acquired perinatally and a birth dose of hepatitis B vaccine given to infants, preferably within 24 hours, has greatly reduced hepatitis B virus transmission from mother to infant(7).
Table II Seroprotection Rate and GMCs for Anti-HBs and Anti-PRP Antibodies
Seroprotection Rate: Antibody concentrations 10 mIU/ml for anti-HBs or 0.15 g/ml for anti-PRP; LL, UL: Lower and Upper Limits of 95% confidence interval; Pre: Pre-vaccination blood sample obtained before Dose 1 of the study vaccine; Post: Post-vaccination blood sample obtained one month after Dose 3 of the study vaccine. The results demonstrated that the vaccine offers 99% seroprotection against hepatitis B infection and 100% seroprotection against H. influenzae type b with a robust increase in GMCs (pre to post blood-sampling time point) for both anti-HBs and anti-PRP antibodies, after the three-dose primary vaccination course. These results are similar to those seen in previous studies (with the same type of vaccine) in terms of seroprotection and GMC values where the seroprotection rate for anti-HBs antibodies ranged from 96% to 100% and for anti-PRP ranged from 98.4% to 100%(8,9). The excellent immunogenicity of the DTP components have been previously demonstrated in other studies conducted across the world(10-12). The study also demonstrated that the vaccine has excellent tolerability profile with only minor adverse events such as local swelling (33.5% of doses) and irritability (29.0% of doses) being commonly reported. Severe adverse events were highly un- common. The incidence of symptoms (solicited/ unsolicited; local/general) observed in this study was similar to those reported in other studies(8,9). Furthermore, the reactogenicity of the combined pentavalent vaccine has been previously demonstrated to be similar to that seen for the DTPw- HBV vaccine or DTPw vaccine when given alone(8). In conclusion, the combined DTPw-HBV/Hib vaccine is immunogenic for the antigens tested, safe and well-tolerated in Indian infants when immunized according to the recommended 6-10-14 weeks schedule. Acknowledgements We thank the doctors and microbiologists who contributed to this study and the Clinical Research Associates, Namitha Krishnamurty and Dr. Murtuza Bughediwala for local monitoring support. We also thank PV Suryakiran for his support in statistical analysis and Preethi Albuquerque and Julia Donnelly for medical writing and editorial assistance. Contributors: SBB, PPM and SDSR were the principal investigators for the study and provided day-to-day supervision of patient enrolment and follow-up and satisfactory conduct of the study. They also provided intellectual input into the preparation of the manuscript. SKD and HLB were involved in conceiving and designing the study and the protocol, and participated in critical review of the manuscript. SKD will also act as guarantor of this paper Funding: GlaxoSmithKline Biologicals, Rixensart, Belgium. Competing interests: Dr. S.K. Datta and Dr. H.L.Bock are employees of GlaxoSmithKline Biologicals.
| ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
References | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
| ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
![]()