|
|
Letters to the Editor Indian Pediatrics 2005; 42:729-730 |
||
|
Bilateral Communicating Intralobar Pulmonary Sequestration |
||
|
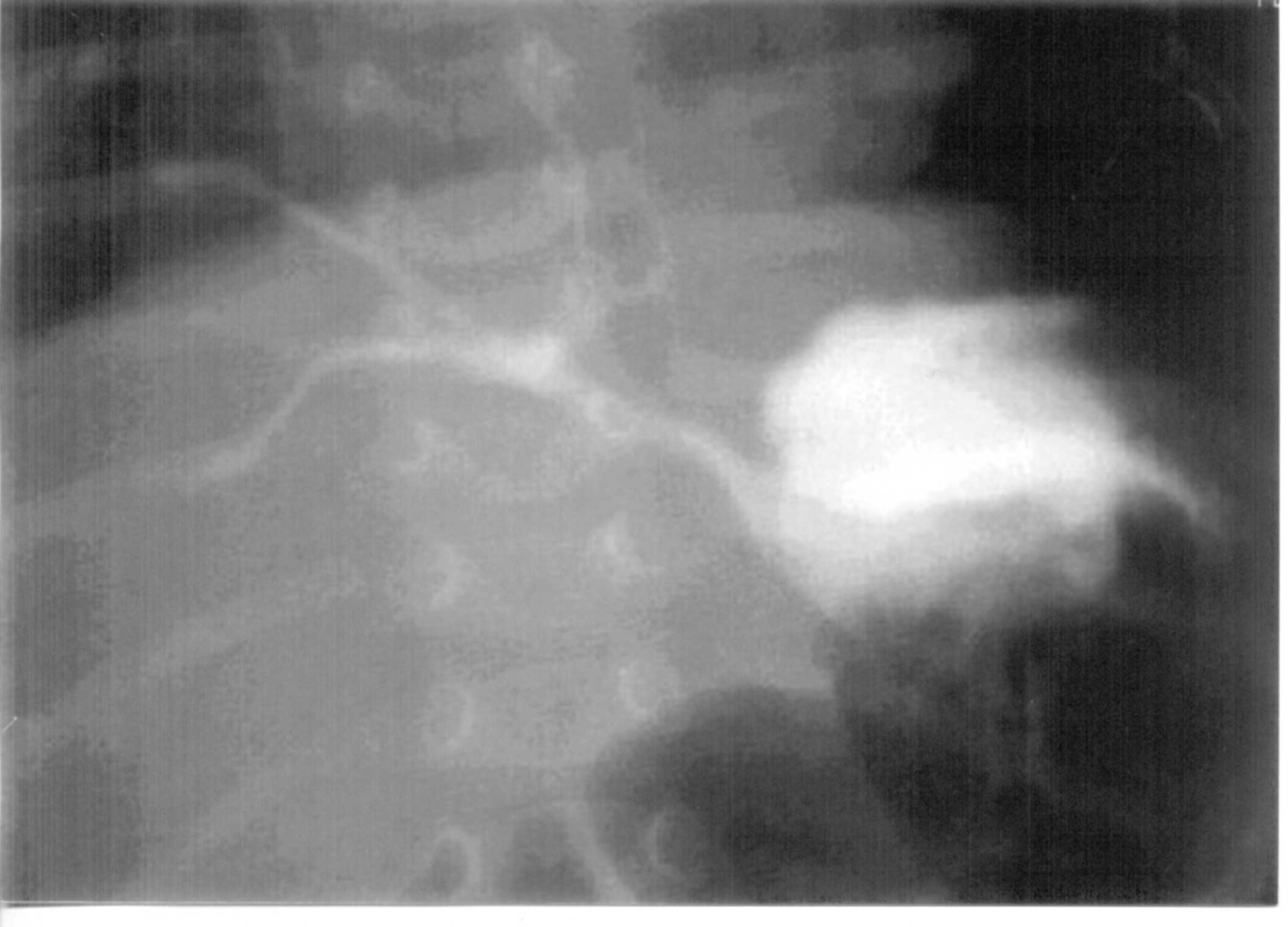
Laparotomy and division of the gastro-bronchial communication was done. Vascular supply was inacessible and so were not divided. Right thoracotomy showed right lower lobe and middle lobe sequestration. Both lobes were resected. Left lower lobe sequestration was left as such since resection of the left lower lobe along with right lower and middle lobes would have caused severe respiratory insufficiency. Vascular supply to the left side was identified and divided. Histopathological examination confirmed the diagnosis of intralobar sequestration. CT scan after 6 months showed that left lower lobe sequestration had disappeared. This is a communicating type of sequestration where the sequestration communicates with the fore gut. Savic, et al.(1) reported that only 2.2% were in the middle or upper lobes. In our case both right and left lower lobes as well as middle lobe were involved making it an extremely rare presentation. Communication through the Pores of Kohn leading to partial aeration of the sequestration was responsible for the partial aeration seen after bronchoscopy. Srikanth, et al.(2) reviewed 57 cases and reported that bilateral communicating sequestrations occurred only in 7% of cases. Treatment consists of lobectomy with division of fistulous communication. Embolisation has been tried with varying results. In our case bilateral lower lobectomies and middle lobectomy would not have been compatible with life. Spontaneous occlusion of the vascular supply has been reported with no untoward effect(3), which prompted us to ligate the blood supply to the left side along with ligation of the gastro-bronchial communication. This combined modality of resection of most infected side with ligation of fistula and vascular supply to the other side may be helpful in similar cases. Acknowledgement We thank Dr. P.K. Rajiv and his team for pre and post-operative medical management in the Department of Neonatology; and Dr. Lakshmi and Dr. Rekha for per-operative anesthetic support. Joy M.G., Department of Pediatric Surgery, Amrita Institute of Medical Sciences, Amrita Lake, Elamakkara, Kochi 682 026, Kerala, India. E-mail: [email protected]
| ||
|
References | ||
|
|
![]()