|
|
Letters to the Editor Indian Pediatrics 2004; 41:749-750 |
|||
|
Diagnostic Dilemma of Cecal Duplication |
|||
|
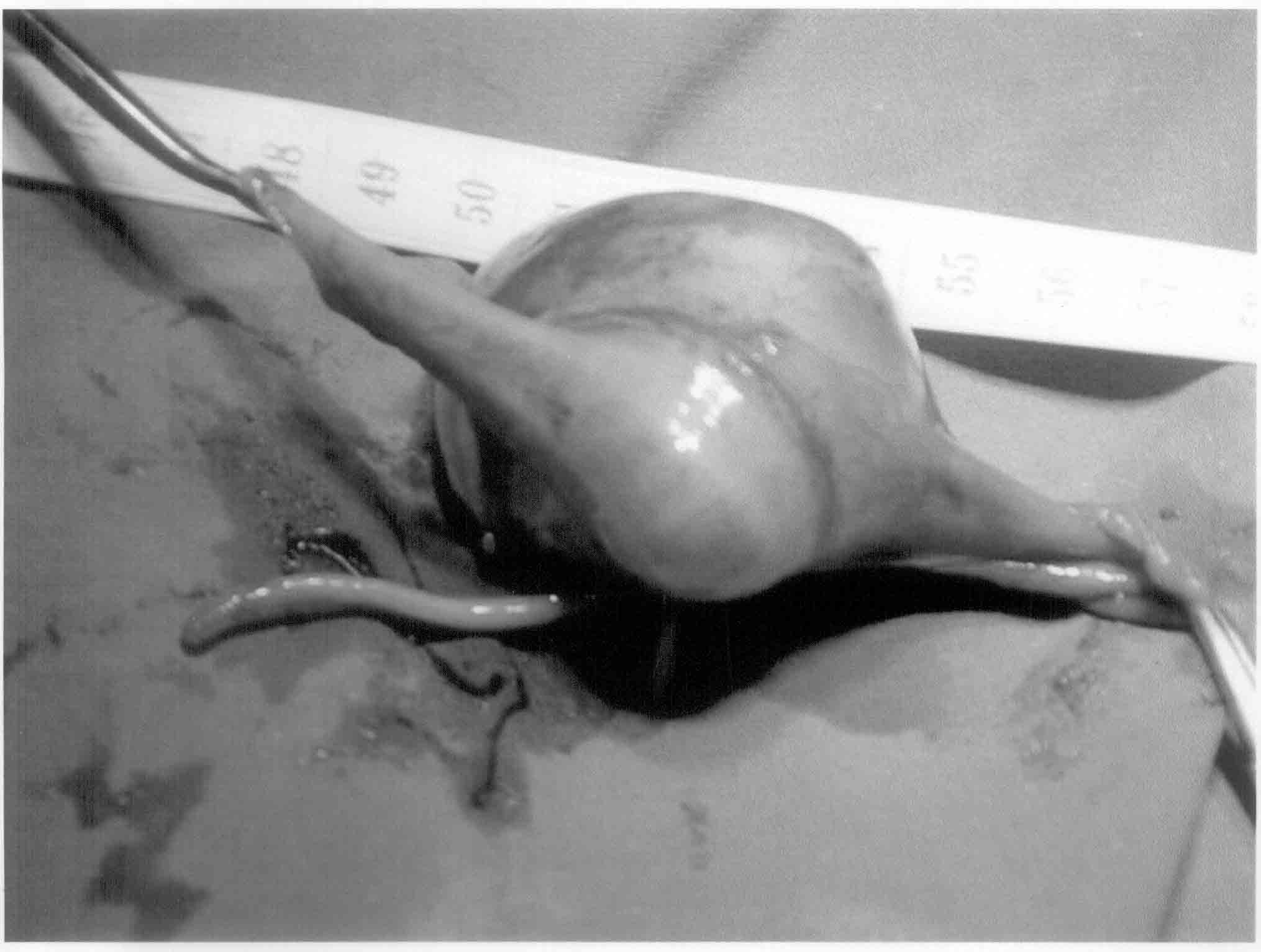
Alimentary tract duplications are rare congenital lesions characterized by intimate attachment to the alimentary tract, presence of well-developed coat of smooth muscle and epithelial lining resembling some part of the alimentary tract(1). Many theories of embryologic origin have been proposed, but the exact etiology has not yet been established. Duplications of the alimentary tract may present at any age, but 80% present in first 2 years of life(2). Only 13% of all alimentary duplications are colonic. Heij, et al.(3) have reviewed 362 patients reported in literature with 400 alimentary tract duplications and found only 16 cases of cecal duplications. Common presenting symptoms are acute intestinal obstruction, vomiting, recurrent abdominal pain, recurrent gastrointestinal bleed, constipation or an incidental detection. In only 20% of cases is a communication found between the gastro-intestinal tract and the duplication. Thirty per cent patients have ectopic gastrointestinal mucosa(4-5). Although ultrasound, CT scan and MRI have been useful, a correct preoperative diagnosis is seldom possible as the symptoms are so varied and the entity rare. Ultrasound shows an echogenic inner mucosal layer with a hyperechogenic outer muscle layer. CT scan shows a well-defined cystic structure with low attenuation and contrast enhancement of the outer rim. Now-a-days, diagnostic laparoscopy may have an important role in the diagnosis of these patients. In the present case, the lesion was cystic and intimately attached to the cecum at the ileocecal junction. Hence, the surgical procedure involved only local resection with a primary anastomosis so as to relieve the patient’s symptoms and prevent recurrence. Cecal duplications may also present as a part of long tubular duplications of the colon which may be treated by either excising the lesion along with the normal colon, enlarging the existing communications with the normal bowel, or by excising a portion of the common wall of the cyst and the normal colon. Although rare, alimentary duplications are an important differential diagnosis to consider in children and especially neonates who present with a palpable abdominal mass. The other possibilities are mesenteric, ovarian, pancreatic or choledochal cysts. Undiagnosed intestinal duplications may cause a bowel obstruction or may undergo malignant transformations in adults. The results of surgical management of duplication depend upon its type, site, extent, attachment to alimentary structures and presence of complications. Amar Shah,
|
![]()