|
|
Brief Reports Indian Pediatrics 2000;37: 771-775 |
||||||||||||||||||||||||||||||||||||||||||||||||||
|
Non-Invasive Estimation of Total Serum Bilirubin by Multi-Wavelength Spectral Reflectance in Neonates |
||||||||||||||||||||||||||||||||||||||||||||||||||
|
Rakesh Lodha
Manuscript received: September 20, 1999; Neonatal jaundice occurs in 70% of term and 80% of preterm babies. Careful monitoring of all jaundiced newborns is required to ensure proper management. Total serum bilirubin (TSB) is commonly determined by spectro-photometric methods by analyzing plasma or serum sample. In addition to need for drawing a blood sample, there is wide range of vari-ability regarding the performance of bilirubin analyzers(1). A large number of studies have demons-trated the possibility of prediction of serum bilirubin in neonates by analysis of the spectral reflectance from the skin(2–8). However, the accuracy of these techniques has been complicated by the variability introduced by skin pigmentation and the dermal maturity; so, the results of studies in white infants may not be applicable to heterogeneous Indian popula-tion. A hand-held transcutaneous bilirubino-meter (BiliCheckTM) has been designed to correct for these interfering factors; being based on recent studies on light scattering characteristics of the human skin(9). This instrument performs a spectral analysis by measuring the intensity of the reflected light at more than 100 individual wavelengths. The major skin components, which impact the spectral reflectance in newborns, are dermal maturity, melanin, hemoglobin and bilirubin(9). By subtracting the spectral contribution of the known components, the bilirubin absorbance is calculated. The present investigation was conducted to determine the clinical accuracy of this Multi-wavelength Spectral Reflectance (MWSR) device (BiliCheckTM) for measuring the transcutaneous bilirubin (TcB) in North Indian newborns.
This study was conducted at the Neonatal Unit of the Department of Pediatrics, AIIMS, New Delhi. Term neonates between ages of 2 and 7 days clinically having icterus more than 8 mg/dl were enrolled in the study. Newborns receiving phototherapy and those who under-went exchange transfusion were excluded. The postnatal age, gestation, birth weight and clinical level of icterus was recorded. TcB measurements were taken on the forehead of each baby using MWSR device. Except for 38 babies, the tip of the instrument (BiliCal) was reused. Within 30 minutes of this estimation, a venous sample was drawn into a glass capillary tube, by another investigator unaware of the above value, for estimating the total serum bilirubin (TSB) value using twin beam Microbilimeter (Ginevri Technologie Biomediche). Both the instruments were cali-brated as recommended by the manufacturers. The data was analyzed using software package Microsoft Excel. The values obtained by Microbilimeter were taken as the gold standard for calculating sensitivity and speci-ficity of transcutaneous bilirubin analyzer and clinical assessment of jaundice by pediatrician. Different tests of agreement were applied. The two sets of values were correlated. In addition the paired differences were calculated and the limits of agreement determined using the method suggested by Bland and Altman(10).
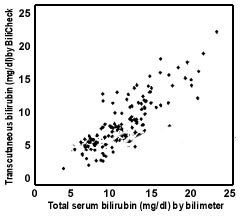
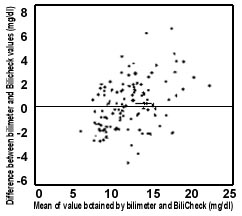
One hundred and nine term neonates with non hemolytic jaundice were included; the mean (SD) gestation and birthweight were 38.4 (1.2) weeks and 2870 (330) grams, respec-tively. The estimations were done at mean (SD) age of 71.8 (27) hours. A total of 121 paired estimations were performed. The TSB values ranged from 4.5 to 21.7 mg/dl. The TcB values correlated fairly with the TSB; the r being 0.823 (Fig. 1). In addition, the mean (SD) paired difference between the TSB and TcB was 0.01 (1.88) mg/dl; the range being –5.1 to 5.8 mg/dl. The 95% limits of agreement were estimated to be –3.6 to 3.6 mg/dl. According to these observations the two values agree poorly (Fig. 2). The sensitivity of TcB to pick up TSB >13 mg/dl was 69%, with a specificity of 89.3% while, with eyes of experienced pediatrician sensitivity of 52.2% and specificity 89.3% was obtained (Table I ). The clinical assessment of icterus correlated better with TcB values (r = 0.84) than with the TSB (r = 0.67). Forty-six babies had TSB greater than 13 mg/dl. In this subgroup the correlation between the TSB and TcB values was poor (r = 0.64). The mean (SD) paired difference between TSB and TcB was 1 (1.7) mg/dl; the 95% limits of agreement being –2.4 and 4.4 mg/dl. We analyzed separately the data for 38 babies where fresh tips were used. The TcB values correlated fairly well with the TSB (r = 0.86). The mean paired difference between the TSB and TcB was 0.5 (1.6) mg/dl; the 95% limits of agreement being –2.7and 3.7 mg/dl. These results are not significantly different from the overall results. Also, the correlation was poor in these babies (n = 16) with bilirubin greater than 13 mg/dl (r = 0.69).
* Clinical judgement can’t differentiate this
group.
Often a pediatrician is interested to corroborate his clinical estimate of icterus with actual serum bilirubin level. Any technique to estimate the level of bilirubin in neonate should ideally be accurate, noninvasive and valid. The results from our study suggest that TcB estimations (BiliCheckTM) agree poorly with the TSB values in heterogeneous North Indian newborn population. Our study suggests that the instrument cannot replace TSB estimations. However, it may be useful as a screening test in centers where trained pediatrician is not available as the TcB correlated fairly well with the clinical estimation. Bhutani et al. reported a high degree of correlation between TcB values (BiliCheckTM) and TSB in American babies(11). At present no other studies are available to confirm these findings. The other transcutaneous bilirubino-meters measure the yellowness of the neonate’s skin, making no allowance for skin maturity or melanin. While these have been shown to be useful in white and certain other populations(2-8), the Indian studies have not been able to show the same degree of accuracy(12–14). Elsewhere also poor correlation has been reported(15). Even the laboratory analyzers have an undesirable intra- and inter-instrument variability(1). We also found that the agreement between TSB and TcB was poor in the subgroup where the TSB was more than 13 mg/dl. Similar results were reported earlier using a different transcutaneous bilimeter(16). The sensitivity of clinical judgement for values >13 mg/dl was poor, though the specificity was good. It seems that the TcB estimation reconfirms the clinical judgement specially for higher bilirubin levels in pathological range (>13 mg/dl). The present study also demonstrated the drawbacks of using correlation as the sole measure of agreement. While the correlation may be good, the difference between the two values may be too large to be acceptable clinically. This has been well highlighted by Bland and Altman(10). In none of the earlier studies, the differences between the two sets of values were looked at. While the manufacturer recommends that the tip (BiliCalTM) be used only once, we reused the tip in majority of the babies. However, the subgroup analysis did not find significant difference between single use and multiple use. We conclude that this TcB instrument may be useful as a screening tool, but it cannot substitute for TSB estimations.
We thank Medisphere Marketing Ltd; New Delhi for providing us the instrument and accessories to conduct the study. Contributors: AKD, VKP coordinated the study (design and interpretation); RL and VJ helped in data collection and RL drafted the paper. AKD will act as the guarantor for the study. Funding: None. Competing: None.
|
||||||||||||||||||||||||||||||||||||||||||||||||||
![]()