|
|
Original Article Indian Pediatrics 2006; 43:14-19 |
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
Cyclosporine in Steroid Dependent and Resistant Childhood Nephrotic Syndrome |
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
Arpana Iyengar, Srilekha Karthik, Anil Kumar, Sharmishtha Biswas and Kishore Phadke From the Children’s Kidney Care Center, Department of
Pediatrics, St. John’s Medical College Hospital, Correspondence to: Dr. K.D.Phadke, Professor of
Pediatric Nephrology, Children’s Kidney Care Center, Manuscript received: October 27, 2004, Initial review
completed: January 4, 2005,
Oral corticosteroids are the first line treatment for a child with idiopathic nephrotic syndrome (INS). Although, most children with INS respond to corticosteroid therapy, 40-90% have subsequent relapses. About one fourth of children with INS have a single relapse, one-third relapse occasionally and one half of them become steroid dependent with a clinical course stretched over many years(1). Steroid dependent nephrotic syndrome (SDNS) is defined as two consecutive relapses, which are not associated with concurrent infections while tapering steroids or within 14 days of stopping therapy. Continuation of long-term steroids in SDNS entails risk of serious side effects. Cyclosporine is another treatment option for children with SDNS. Steroid resistance (SRNS) is defined as failure to achieve remission inspite of four weeks of prednisolone in the dose of 60 mg/m2/day. Various modalities of treatment have been used in these patients including pulse methylprednisolone, alkylating agents like cyclophosphamide or chlorambucil, pulse methyl prednisolone plus alkylating agents, cyclosporine, FK-506, mycophenolate mofetil, etc. Results obtained with these drugs are often contradictory and difficult to analyze. Also, the cost limits their use in our country. Thus, children with SDNS and SRNS pose therapeutic challenges. We report our experience with CyA monotherapy in these and analyze variables predicting response and outcome. Subjects and Methods Forty-one patients who received CyA monotherapy were studied. Thirty children had SONS and 11 had SRNS. Patients with SRNS had initial resistance, normal renal functions and were normotensive. They had received at least one course of cytotoxic drugs. All were subjected to kidney biopsy prior to CyA therapy. None of these children received antiproteinuric drugs like ACE inhibitors or angiotensin receptor blockers. The criteria for diagnosis of nephrotic syndrome, relapse, remission, SDNS and SRNS were as per the definitions used by the International Study of Kidney Diseases in Children(2). CyA was used at a dosage of 6-7 mg/kg/day, either in oral solution form or capsules in two divided doses. In SDNS CyA was started when they were in remission. Steroids were tapered over the next 1-2 months in these patients. Concurrent steroids were not used in order to minimize risk of infection due to added immunosuppression. Favorable response meant complete clinical and biochemical remission (proteinuria <1 g/m2/day or protein/creatinine ratio on a random urine sample < 2.5) on CyA therapy lasting as long as the same dose was administered. CyA dosage was adjusted according to blood levels in these patients, the target levels being 100-200 ng/mL (fluorescent polarization immuno-assay). In CyA responders, attempt was made to gradually taper to the minimum dosage required to keep them in remission. CyA resistance was defined as a lack of remission after 3 months of CyA therapy. CyA dependence was defined as the occurrence of relapse while on CyA or within one month of stopping treatment. All patients were monitored for toxicity by serial assessment of renal and hepatic functions every 2-4 weeks initially for first two months and later every three months. Serially, assessment of urine spot protein/ creatinine ratios, 24 hour proteinuria, serum albumin and cholesterol were done. First ten patients had repeat kidney biopsies after two years of therapy. No specific changes that could be attributed to CyA toxicity could be identified on repeat biopsies. Intercurrent infections were managed appropriately without changing CyA dosage. Significant infections like pneumonia, peritonitis and cellulitis were recorded. CyA was discontinued in the presence of deteriorating renal functions defined as a consistent rise in serum creatinine >0.3 mg/dL above its baseline. Statistical Methods Statistical analysis was done using SPSS package for Windows (version 10.0 SPSS). The endpoints were response to CyA (responders / non-responders), CyA dependence, occurrence of significant infections requiring hospitalizations and development of chronic renal failure. Time of CyA usage from onset of NS was categorized into groups of 3-9, 10-14, 15-42 and 43-240 months. Variables including age of patient at onset, the time interval between the onset and CyA usage, steroid response and biopsy findings were examined against the above end points using univariate and multivariate analysis; P<0.05 was considered significant (two-tailed). Association of CyA response with the variables was tested using Pearson-Chi-square test (Table I). Logistic regression model was applied to determine the chance of a favorable CyA response in relation to the variables. Table I
MCNS: Minimal change rephrotic syndrome; SDNS: Steroid dependent
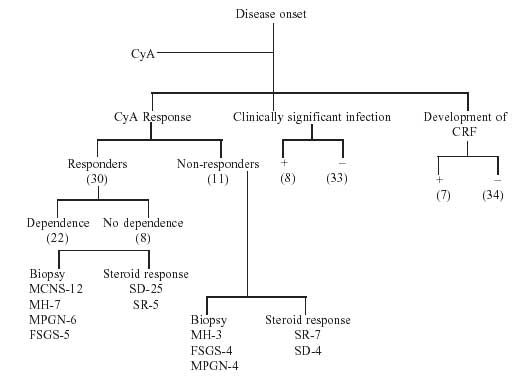
nephrotic syndrome; Results Of 41 patients, 30 were boys, 11 girls. The median age of patients was 93 months (range 48-936) months. The median age at onset of NS was 22 months (range 11-148) months. Time of CyA usage from onset of NS was 16 months (range 3-156) months. Median duration of CyA usage was 24 (range 6-72) months. The median follow up period was 71 months (range 20 -205 months). On biopsy, 13 children had MCNS (11 SDNS, 2 SRNS), 10 had mesangial hypercellularity (6 SDNS, 4 SRNS), 10 had MPGN (7 SDNS, 3 SRNS) and 8 had FSGS (5 SDNS, 3 SRNS). Eleven children were CyA resistant of which 4 children had FSGS and MPGN each while three had mesangial hypercellularity (Fig. I). Seven of these eleven children were resistant to steroids while four were dependent on steroids. Out of the remaining 30 who were CyA responders, 22 (73.33%) had CyA dependence. On univariate analysis, favorable CyA response had a significant direct association with steroid response (P=0.003), MCNS on biopsy (P = 0.008) and earlier use of CyA (P = 0.022). Age of onset at NS was not associated with CyA response (P = 0.163). Since on univariate analysis the independent variables were significant, a multivariate analysis was done. In logistic regression model only shared responsiveness emerged as a significant predictor of CyA response c2 8.6; (OR = 95%, CI = 1.2-56.4, P = 0.003) (Table I).
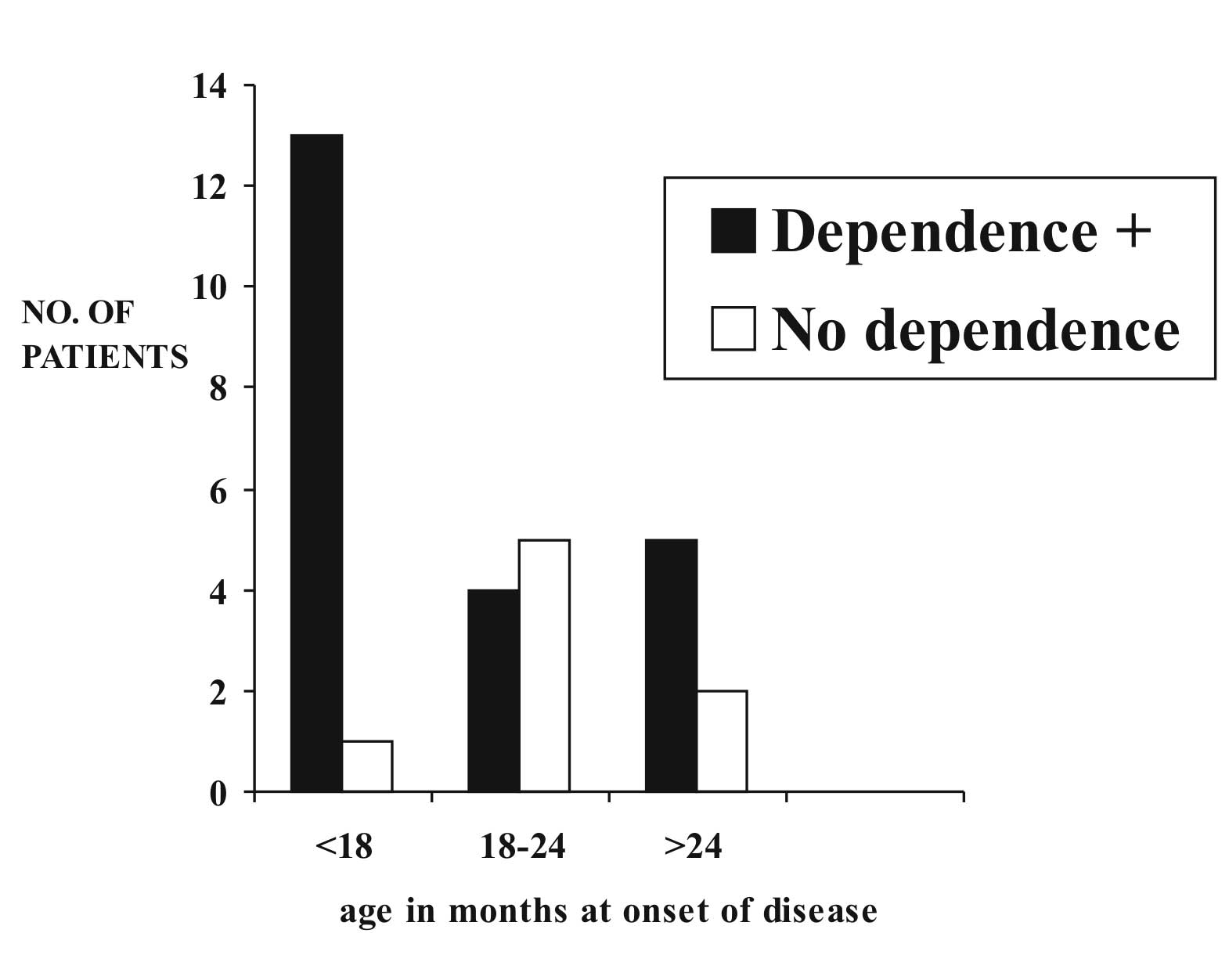
Development of CyA dependence showed a significant direct association (P = 0.022) with age of onset of the disease (Fig. 2). Favorable CyA response showed a significant association with less instances of development of clinically significant infection (P = 0.02). CyA response (P = 0.000) showed significant direct association with development of CRF.
Discussion CyA is now a well-recognized treatment for patients with SDNS and SRNS. Unfortunately CyA induced remission is not long lasting and CyA dependence is a major problem. Very few studies have tried to analyze variables predicting response to CyA and outcome in these children. The response to CyA has been correlated more with steroid response than with underlying histo-pathology(3). Niaudet, et al. describe a remission rate of 48% among patients with MCNS and 30% of patients with FSGS(4). The duration of CyA therapy was however short (mean 9.6 weeks) in that study. Twenty-seven children out of 42 with SRNS responded to CyA in their series. Singh, et al. reported good CyA response in (59.5%) patients with FSGS and in 83% patients with MCNS(5). Increased glomerular or interstitial scarring on a pre-CyA renal biopsy tends to correlate with a poorer response to CyA(6). In our series, all children with MCNS whereas only 60.7% of non-MCNS responded to CyA. Although steroid responsiveness, MCNS and earlier use of CyA seem to point to likelihood of favorable CyA response, the age at onset of disease did not seem to have such association. On multivariate analysis however, only steroid responsiveness emerged as a significant factor predicting favorable CyA response. Poorer response to CyA in younger patients could perhaps be explained by the twice-daily CyA regimen. In our series, all patients received twice daily CyA regimen. In retrospect, younger children could have received thrice a day dose schedule. Others have reported 100% CyA dependence in SDNS(7). Takeda, et al. suggested that the children who relapse after CyA therapy may experience a worse relapsing course compared to after cyclophosphamide or chlorambucil(8). In our series, 73.3% of CyA responders became CyA dependent. Younger age at onset of the disease was significantly associated with development of CyA dependence. Expectedly, the risk of developing significant infections was significantly higher in CyA non-responders compared to responders. This would have an important bearing on practical management of these children. Development of CRF is a dreaded complication of refractory nephrotic syndrome. Singh, et al. reported 83 children with refractory NS secondary to a wide spectrum of glomerular diseases(5). Twenty among these reached end stage renal disease over a 10-year period. Ingulli, et al postulated that long term CyA therapy blunts the progression of FSGS to ESRD(9). In our series, none of CyA responders developed CRF, at least upto a mean follow-up period of 71 months. It is unclear at present as to how long CyA treatment should be continued. Long-term studies in this regard will hopefully provide answers. High cost of CyA may be a limiting factor for its widespread use in our country. In conclusion, the predictors for CyA non-responsiveness are steroid resistance, non-MCNS on renal biopsy and longer duration between onset of nephrotic syndrome and usage of CyA, irrespective of the age at onset of the disease. There is a high incidence of CyA dependence among young responders. Children who are CyA resistant are at high risk to develop significant infections and CRF. Contributors: KDP was involved in designing the study and preparation of the manuscript. He will act as guarantor of the study. AI, AK were involved in data collection. SK has helped in manuscript writing. SB collected and analyzed the data. Funding: None. Competing interests: None stated.
| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
References | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
![]()