|
Images in Clinical Practice |
Indian Pediatrics 2000;37: 103-104 |
Primary Empty Sella Syndrome |
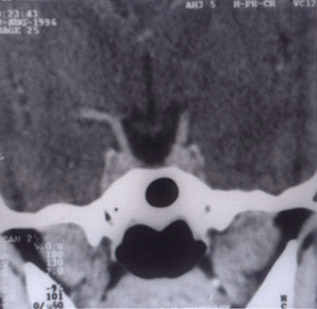
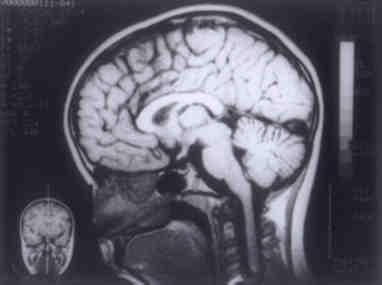
A 12�-year-old girl presented with polyuria, polydipsia and poor gain in height for 4 years. She had average scholastic performance. She had constipation. Menarche had not been attained. There was no history of head injury, seizures, alteration of sleep, visual symptoms, headache or polyphagia. There had been no perinatal problems. She weighed 24.5 kg and was 128 cm tall. Arm span was normal. Upper and lower segments were equal. There was no goiter. Vital signs were normal while BP was 100/60. Carrying angle was normal. Puberty staging was Tanner stage 1. Ankle jerks showed delayed relaxation. Perimetry and acquity of vision were normal. Bone age was approxi-mately 10 years. Water deprivaton test was suggestive of central diabetes insipidus. Hormo-nal assay showed low T3, T4 and TSH. Skull X-ray showed an enlarged sella. CT scan head (Fig. 1) showed enlarged sella filled with CSF with small pituitary gland pushed upwards. MRI (Fig. 2) confirmed these findings. Also, there was an indentation on the undersurface of the compressed pituitary. Hence, a diagnosis of pri-mary empty sella syndrome (PESS) was made.
Fig. 1. Contrast enhanced CT scan head in coronal section taken through pituitary fossa shows small pituitary gland lying in the upper part of sella turcica which is filled with CSF.
Fig. 2. T1 weighted MRI brain in midsagittal section shows small pituitary gland which is compressed from below by CSF inside the sella turcica. The term empty sella is applied when the diaphragm sella is incompetent and subarach-noid space with CSF herniates into the sella, compressing the pituitary and enlarging the sella. Where there is no prior history of inter-vention for a pituitary tumor, the condition is called PESS. Empty sella may remain asympto-matic. The typical presentation is of an obese middle-aged woman with headache. Endocrino-pathy is more common in children then in adults who have neurologic signs and symptoms more often. Visual symptoms and associated cranio-facial anomalies may also occur in children. PESS is usually associated with pituitary hypo- function but can also be found in those with hypo-thalamo-pituitary hyperfunction. Involve-ment of the posterior pituitary as in this case, is however rare. Multiple factors may contribute to the formation of an empty sella including diaphragmatic incompetence, raised intracranial pressure, arachnoid cysts and spontaneous abla-tion of pituitary by infarction or hemorrhage. Symptomatic medical therapy is most often resorted to; rarely surgical intervention is required for PESS. Sudeshna Mitra, |