Tracheobronchial foreign body aspiration can occur in
all age groups but is more common in children. A previously healthy
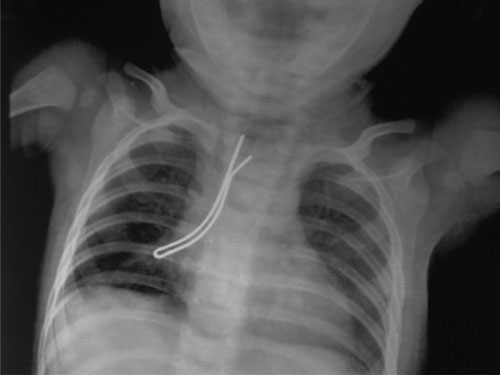
5-month-old child presented to our hospital with aspiration of a
metallic hair pin, one day before. As per the parents, the elder male
sibling (3 years old) was playing with the child when the patient
accidentally aspirated the hair pin. This was immediately followed by
cough.
The child was restless with minimal respiratory
distress, pulse rate 140/min and SpO
Airway foreign bodies lead to significant morbidity
and pose a risk of death in the pediatric population because of their
small airways [1]. Rigid bronchoscopy is the gold standard for diagnosis
and treatment of inhaled foreign body in children [2]. Even in the hands
of experienced endoscopists, there may be occasions when an endoscopic
approach to airway foreign bodies should be abandoned in favour of an
open surgical procedure [3]. The need for open surgical intervention
ranges from 0.3-4% in various published series [3,4]. Tracheostomy for
removal of tracheobronchial foreign bodies, as described for our
patient, is reported in very few cases in the literature [5,6]. The
child being 5 months old and the foreign body being large, with pointed
sharp ends facing the glottis and base of tongue, made this case
surgically challenging.
1. Tan HKK, Brown K, McGill T, Kenna MA, Lund DP,
Healy GB. Airway foreign bodies: A 10-year review. Int J Pediatr
Otorhinolaryngol. 2000; 56:91-9.
2. Farrell PT. Rigid bronchoscopy for foreign body
removal: Anaesthesia and ventilation. Paediatr Anaesth. 2004;14:84-9.
3. Ulku R, Onen A, Onat S, Ozcelik C. The value of
surgical approaches for aspirated pen caps. J Pediatr Surg.
2005;40:1780-3.
4. Zhijun C, Fugao Z, Niankai Z, Jingjing C.
Therapeutic experience from 1428 patients with pediatric
tracheobronchial foreign body. J Pediatr Surg. 2008;43:718-21.
5. Marks SC, Marsh BR, Dudgeon DL. Indications for
open surgical removal of airway foreign bodies. Ann Otol Rhinol Laryngol.
1993;102:690-4.
6. Fraga JC, Neto AM, Seitz E, Schopf L. Bronchoscopy
and tracheotomy removal of bronchial foreign body. J Pediat Surg.
2002;37:1239-40.