Infants put almost everything into their mouths and toddlers eat just
about anything. The majority of foreign body ingestions occur in
children between the ages of six months and three years [1]. Only 10 to
20 percent of foreign bodies require endoscopic removal, and less than 1
percent require surgical intervention [1,2].
 |
|
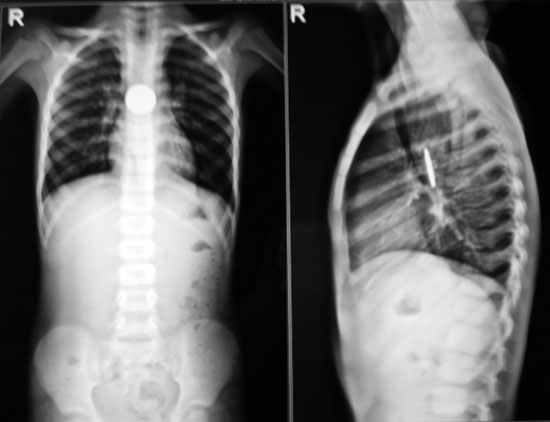
Fig. 1 X-ray chest PA and Lateral view
showing radio-opaque foreign body.
|
Retained foreign body in esophagus is very rare
presentation, which may damage the mucosa leading to stricture or
fistula. We report a case of 8-yr-old male child who was brought to
medical attention with complaints of vomiting after meals and difficulty
in swallowing food for the past 4 years, along with cough and noisy
breathing for three months. There was a history of ingestion of a
2-rupee coin prior to start of the symptoms, passage of which the
parents never noticed subsequently in stools, and they did not seek any
further medical attention. After admission, X-ray chest was done
which revealed a radio-opaque shadow in the mid esophagus; lungs were
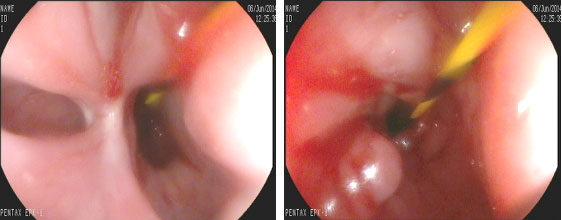
normal (Fig. 1). Upper gastrointestinal endoscopy revealed
a stricture at 12 cm from incisors; proximal esophagus showed
diverticulum and the coin was seen distal to the stricture. The
stricture was dilated using Savory Gillard dilators and the coin was
pushed distally into the stomach. (Fig 2). A contrast X-ray
swallow (gastrograffin) study was normal. After one week, the child
passed the coin in the stool. Repeat dilatation was done after 7 days
and 21 days. After dilatation, the child started accepting feeds orally
without any complaints; there was no requirement of dilatation after
three initial sessions.
 |
|
Fig. 2 Stricture and diverticulum in
esophagus.
|
Retained esophageal foreign bodies are uncommon in
pediatric practice and they should be endoscopically removed as soon as
possible. In our patient, the appropriate management for coin ingestion
was not done at the time of ingestion and thus led to retained foreign
body and stricture formation. Esophageal stricture resulting from a
long-standing lodgment of metallic foreign bodies has been reported
earlier [3,4]. As retained esophageal foreign body can lead to
stricture, a timely appropriate management should be done at the time of
ingestion.
1. Wyllie R. Foreign bodies in the gastrointestinal
tract. Curr Opin Pediatr. 2006; 18:563.
2. Uyemura MC. Foreign body ingestion in children. Am
Fam Physician. 2005; 72:287.
3. Doolin EJ. Esophageal stricture: An uncommon
complication of foreign bodies. Ann Otol Rhinol Laryngol.
1993;102:863-6.
4. Sheen TS, Lee SY. Complete esophageal stricture
resulting from a neglected foreign body. Am J Otolaryngol.
1996;17:272-5.


