|
|
|
Indian Pediatr 2014;51:
145-146 |
 |
Granulocytic Sarcoma of the lung in Acute
Myeloid Leukemia
|
|
Rajat Thawani, Akanksha Chichra, Amita Mahajan and *Lata Jadhav
From the Departments of Pediatrics and *Pathology,
Indraprastha Apollo Hospital, New Delhi, India.
Correspondence to: Dr Rajat Thawani, F-61/B,
Gangotri Enclave, Alaknanda, New Delhi 110 019, India.
Email: [email protected]
Received: August 11, 2013;
Initial review: September 03, 2013;
Accepted: November 27, 2013.
|
|
Background: Granulocytic sarcoma, an uncommon solid, extra-medullary
tumor is a rare presentation of acute myeloid leukemia. Case
characteristics: A seven-year old boy admitted to the hospital for
treatment of leukemia having radiological findings of consolidation in
one lung. Observation/Intervention: A bronchoalveolar lavage was
done which was negative for tubercular, bacterial, and fungal infection
but showed blast cells. Outcome: On day seven of chemotherapy, a
repeat chest x-ray showed resolution of the lesion. A high-resolution
Computerized tomography of chest repeated after one month of induction
showed resolution. Message: A consolidation on chest radiograph
in acute myeloid leukemia can be a granulocytic sarcoma of the lung; a
bronchoalveolar lavage may be offered to confirm or refute this
diagnosis.
Keywords: Acute myeloid leukemia,
Bronchoalveolar lavage, Sarcoma.
|
|
Granulocytic sarcoma is a solid, extra-medullary
tumor comprising of granulocytic precursor cells. It is a rare
presentation of acute myeloid leukemia (AML). The most common sites of
involvement are the skin, bone, soft tissue and lymph node. We report a
child with granulocytic sarcoma of the lung.
Case Report
A seven-year-old boy was referred to our hospital
with history of fever and cough for the past ten days along with
bodyache and fatigue for the past three days. His peripheral blood smear
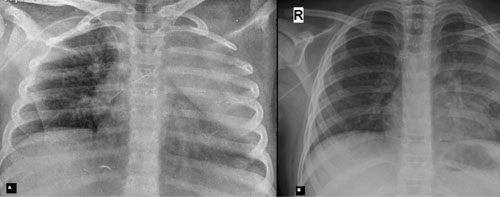
done elsewhere had blast cells. His chest X-ray showed left upper
zone opacity (Fig. 1).
 |
|
Fig. 1 Image showing chest X-ray
before (a) and seven days after (b) induction chemotherapy.
|
He was admitted to our hospital; a complete blood
count revealed hemoglobin of 8.8 g/dL, total leucocyte
count of 50,500/mm3
and platelet count of 50,000/mm3.
Bone marrow was replaced by blasts. His cerebrospinal fluid was also
positive for malignant cells. Immunopheno-typing confirmed blasts to be
positive for CD13, CD33, CD14, CD34 and HL-DR. This was consistent with
M4 subtype of acute myeloid leukemia. Karyotype was normal and
cytogenetics were negative for t (8; 21), PML-RARA, inv (16) and
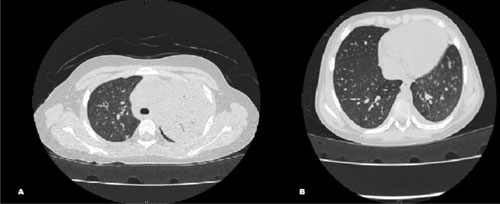
monosomy 7. High-resolution computerized tomography (CT) of chest showed
left upper lobe consolidation with centrilobular nodules (Fig.
2).
 |
|
Fig. 2 Image showing HRCT chest before
(a) and one month after (b) induction chemotherapy.
|
Broad-spectrum antibiotics and voriconazole were
started empirically. A bronchoalveolar lavage (BAL) done on day two of
admission was hemorrhagic and mucoid. No bacteria or fungus was detected
on microscopy and culture. Galactomannan was negative in the BAL fluid.
Microscopy showed atypical round cells with round cleaved nucleus and
scanty rim of cytoplasm, similar to those seen in blood and bone marrow
examination. The cells were myeloperoxidase positive suggestive of blast
cells. There were no reactive cells. A diagnosis of granulocytic sarcoma
of the lung was made and chemotherapy was started as per AML 15
protocol. He received daunorubicin 50 mg/m2
by slow intravenous push on day 1, 3 and 5, and cytosine arabinoside 100
mg/m2 12 hourly by
intravenous push on days 1 to 10.
On day seven of chemotherapy, a repeat chest X-ray
showed resolution of the lesion (Fig. 1). A high
resolution CT of chest repeated after one month of induction also showed
resolution (Fig. 2).
Discussion
Granulocytic sarcomas are uncommon extra-medullary,
solid tumors composed of granulocytic precursor cells. The most common
sites for these are skin, bone, soft tissue and lymph node [1]. It is
commonly associated with acute myeloid leukemia, but it may indicate
leukemic transformation in myelodisplastic disorders, chronic myeloid
leukemia, myelofibrosis, polycythemia vera or chronic eosinophilic
leukemia [2,3]. Granulocytic sarcoma does not seem to have any
prognostic significance in acute leukemia [4].
Granulocytic sarcoma in the lung is a rare entity
[4]. In our case, the patient had an opacity visible in his chest X-ray
and CT scan. Such focal masses during the course of acute myeloid
leukemia may be an infection, hemorrhage or secondary neoplasms, apart
from a granulocytic sarcoma [5]. It is known to be confused with
opportunistic infections of the lung [6,7]. A diagnosis of granulocytic
sarcoma is usually based on its appearance, location and a concurrent
diagnosis of AML [8]. The tissue confirmation is done by morphology, and
with stains like myeloperoxidase, periodic-acid schiff and neuron
specific enolase [8]. The appearance of myeloblasts can range from well
differentiated to poorly differentiated within a granulocytic sarcoma
[9]. In our child, a possibility of fungal and bacterial infection was
considered but BAL showed blast cells confirming the diagnosis of
granulocytic sarcoma.
We conclude that a consolidation on chest radiograph
in acute myeloid leukemia can be a granulocytic sarcoma of the lung; a
bronchoalveolar lavage may be offered to confirm or refute this
diagnosis.
References
1. Thachil J, Richards RM, Copeland G. Granulocytic
sarcoma - a rare presentation of a breast lump. Ann R Coll Surg Engl.
2007;89:W7-9.
2. Liu PI, Ishimaru T, McGregor DH, Okada H, Steer A.
Autopsy study of granulocytic sarcoma (chloroma) in patients with
myelogenous leukemia, Hiroshima-Nagasaki 1949-1969. Cancer.
1973;31:948-55.
3. Neiman RS, Barcos M, Berard C, Bonner H, Mann R, Rydell
RE, et al. Granulocytic sarcoma: a clinicopathologic study of 61
biopsied cases. Cancer. 1981;48:1426–37.
4. Guermazi A, Feger C, Rousselot P, Merad M, Benchaib
N, Bourrier P, et al. Granulocytic sarcoma (chloroma): imaging
findings in adults and children. AJR. American J Roentgenol.
2002;178:319-25.
5. Pui MH, Fletcher BD, Langston JW. Granulocytic
sarcoma in childhood leukemia: imaging features. Radiology.
1994;190:698–702.
6. Guimarães MD, Marchiori E, Marom EM, Routbort MJ,
Godoy MCB. Pulmonary granulocytic sarcoma (chloroma) mimicking an
opportunistic infection in a patient with acute myeloid leukemia. Ann
Hematol. 2013:10–11 (E-pub ahead of print).
7. Takasugi JE, Godwin JD, Marglin SI, Petersdorf SH.
Intrathoracic granulocytic sarcomas. J Thorac Imaging. 1996;11:223-30.
8. Lee DA, Harris CP, Gresik VM, Rao P. Granulocytic
sarcoma presenting as pneumonia in a child fluorescent in situ
hybridization. J Pediatr Hematol Oncol. 2004;26:431-4.
9. Menasce LP, Banerjee SS, Beckett E, Harris M.
Extra-medullary myeloid tumour (granulocytic sarcoma) is often
misdiagnosed: a study of 26 cases. Histopathol. 1999;34:391-8.
|
|
|
 |
|
