|
|
|
Indian Pediatr 2013;50: 257 |
 |
Descemet Membrane Breaks Following Forceps
Delivery
|
|
Suma Ganesh, Priyanka Arora and *Kamaldeep Arora
Department of Pediatric Ophthalmology and Strabismus,
Dr Shroff’s Charity Eye Hospital; and
Department of Pediatrics, All India Institute of Medical Sciences, New
Delhi, India.
Email:
[email protected]
|
|
A term male neonate born by forceps vaginal delivery presented on day 10
of life with watering and opacification of cornea of left eye. There was
associated lacrimation, photophobia and blepharospasm. Eye examination
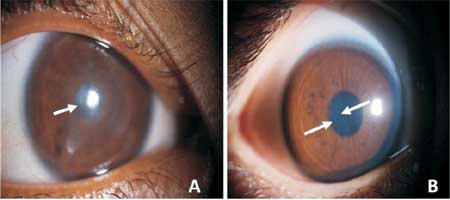
under anaesthesia revealed corneal edema (Fig.1) with
normal intraocular pressure. Corneal edema resolved following topical
corticosteroids but on repeat examination vertically oriented breaks
were noted in descemet membrane (Fig.2b, white double
arrow). These breaks were associated with myopic astigmatism of 3.50 D
along the axis of break. Refractive correction was prescribed along with
standard occlusion therapy. At follow up of 2 months and later at 2
years, refractive error was stable with the best corrected visual acuity
of 20/30 in the affected eye.
 |
|
Fig.1 Slit lamp photographs of
affected (left) eye; Panel A: on 10th day of life revealing
diffuse corneal edema (white arrow); Panel B: On day 28 of life
revealing vertical break at the level of descemet’s membrane
(white, double arrow).
|
Forceps injury to eye usually occurs as a result of
compression of the globe between the orbital roof and the blade of the
obstetric forceps. It is associated with descemet membrane breaks and
can cause refractive errors. These breaks being small and obscured by
corneal edema are easily missed. A normal intraocular pressure
facilitates differentiation from congenital glaucoma. The corneal edema
improves within a few weeks, at which time residual single or multiple
descemet membrane breaks appear as vertical or oblique median striae.
These corneal lesions are primarily unilateral and may cause amblyopia.
Loss of vision may be because of the opacities of the striae themselves
or because of induced astigmatism, which results in amblyopia. Although
penetrating keratoplasty has been the treatment of choice, but this
leads to frequent complications in children.
|
|
|
 |
|
