|
|
|
Indian Pediatr 2012;49: 145-146
|
 |
Corrosive Tracheo-esophageal Fistula Following
Button Battery Ingestion
|
|
MM Harjai, WVBS Ramalingam,
#G
Chitkara and #A Katiyar
From the Department of Surgery and Paediatric Surgery,
Command Hospital (Southern Command) Pune 411 040, Maharashtra; and
Department of Otorhinolaryngology, and #Department of Surgery, Army
Hospital (Research & Referral), Delhi Cantt, New Delhi 110 010, India.
Correspondence to: Colonel Man Mohan Harjai, Professor, Senior Advisor
Surgery and Paediatric Surgery, Command Hospital, (Southern Command),
Pune 411 040, Maharashtra, India.
Email: [email protected]
Received: October 03, 2010;
Initial review: October 07, 2010;
Accepted: October
28, 2010.
|
We describe a case of corrosive tracheo-esophageal fistula following
button battery ingestion in a 1-year old nonverbal pediatric patient.
The delay in diagnosis was caused by failure to obtain correct history
and failure to detect opacity of the battery in the neck at the first
visit. The large fistula was successfully treated with division and
repair with non absorbable sutures, with interposition of strap muscles
between separated trachea and esophagus.
Key words: Button battery, Corrosive ingestion, Ingestion,
Tracheo-esophageal fistula.
|
|
Tracheo-esophageal fistula following a foreign
body impaction in the esophagus is a rare and serious complication.
We report consequences of an unrecognized button battery impaction
in the esophagus, which resulted in tracheo-esophageal fistula
formation and was not diagnosed for more than 18 days due to
masquerading of button battery shadow by haziness of associated
pneumonia.
Case Report
One year old child was taken to a private
practitioner by the parents for sudden onset of hoarseness of voice.
He was treated as a case of acute laryngitis. When symptoms of high
grade fever, cough, change in voice and drooling persisted for 10
days, baby was brought to the emergency room of a peripheral
hospital. The chest radiograph revealed hazy opacities all over both
lung fields with unclear cervical region. A diagnosis of acute
laryngotracheobronchitis was made and patient treated accordingly.
However, patient was not maintaining saturation and developed
cyanosis. He was placed on ventilatory support along with broad
spectrum antibiotics and other supportive measures. Patient showed
signs of improvement after 48 hours and was extubated after 72
hours. Even after extubation patient did not show expected
improvement. He had persistent excessive drooling of saliva with
increased cough on swallowing and had episodes of desaturation. On
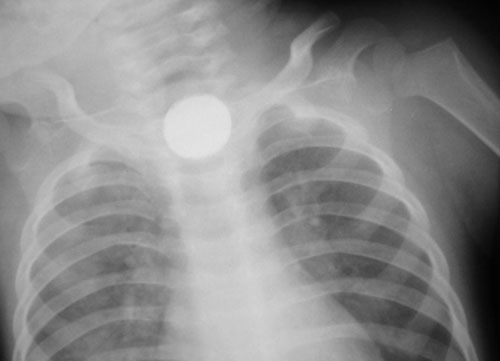
18 th day of illness a
fresh chest skiagram showed a hitherto unnoticed round opacity in
the neck region (Fig. 1). A possibility of
foreign body impacted in the esophagus was considered. Review of old
skiagram of chest, the same opacity was now be discerned. The
foreign body was extracted with the help of a rigid esophagoscope.
It was a button battery of 1.5 cm diameter from a toy electronic
harmonium. The symptoms persistently increased even after removal of
button battery. Patient was transferred to our centre with a
provisional diagnosis of esophageal stricture. Contrast study
revealed spill of dye in the lung fields. A diagnosis of acquired
tracheo-esophageal fistula secondary to button battery impaction was
made. A upper gastrointestinal endoscopy revealed a large wide
fistula at the level of thoracic one vertebrae. The endotracheal
tube was clearly visible from the esophageal side. In view of wide
fistula in a symptomatic child, decision of primary closure of the
fistula was taken. The fistula was divided and repaired with non
absorbable sutures with interposition of strap muscles between
separated trachea and esophagus. He was kept on elective ventilation
for 48 hours. Post operative period was uneventful.
 |
|
Fig. 1 Skiagram chest showing
appreciable button battery shadow in the neck region on 18 th
post-ingestion day.
|
Discussion
In our patient, a wide tracheo-esophageal fistula
developed due to the presence of impacted foreign body for 20 days.
In this child, button battery must have lodged or impacted for
tissue damage to occur. The esophagus is especially susceptible to
foreign body retention due to its several anatomic areas of
narrowing and weak peristalsis [1,2]. The tissue damage that result
from contact with charged battery is a chemical burn caused by
production of sodium hydroxide (cathode) and hydrochloric acid
(anode) generated from electric current passing through physiologic
electrolyte solution [3]. Failure to recognize or appropriately
manage a foreign body in the oesophagus may lead to complications
and occasional mortality. Management approaches include endoscopic
or open surgical repair. Unfortunately, these procedures can be
complicated by high rates of recurrent laryngeal nerve injury,
tracheal stenosis, recurrent fistula and significant patient
mortality. These fistulae can be managed conservatively by use of
esophageal rest to permit closure by secondary intention [4].
However, we did a primary repair of tracheo-esophageal fistula with
interposition of strap muscles of neck as we found on upper
gastrointestinal endoscopy that the margins of fistula were healthy
and the fistula was very wide, which was unlikely to close
spontaneously.
Contributors: All contributors have
participated sufficiently in the intellectual content, conception
and design of this work, as well as the writing of the manuscript,
to take public responsibility for it and have agreed to have their
name listed as a contributors.
Funding: None; Competing interests:
None stated.
References
1. Hamilton JM, Schraff SA, Notrica DM. Severe
injuries from coin cell battery ingestions: 2 case reports. J
Pediatr Surg. 2009;44:644-7.
2. Bernstein JM, Burrows SA, Saunders MW. Lodged
oesophageal button battery masquerading as a coin: an unusual cause
of bilateral vocal cord paralysis. Emerg Med J. 2007;24:e15.
3. Sigalet D, Lees G. Tracheoesophageal injury
secondary to disc battery ingestion. J Pediatr Surg. 1988;23:996-8.
4. Grisel JJ, Richter GT, Casper KA, Thompson DM. Acquired
tracheoesophageal fistula following disc-battery ingestion: can we
watch and wait? Int J Pediatr Otorhinolaryngol. 2008;72:699-706.
|
|
|
 |
|
