Neurotuberculosis presenting as space occupying lesion
(tuberculoma) within the brain parenchyma is commonly encountered in
developing countries [1]. Tuberculomas occur due to hematogenous spread
and are generally intra-parenchymal in location with extra-axial and
intra-ventricular locations being rare [1-4]. We present a rare case of
fourth ventricular tuberculoma.
A four-and-half year old female child presented in a
semiconscious condition with a history of progressive severe headache,
vomiting and double vision for one week and low grade fever for two
months. There was no past history of tuberculosis. Fundus examination
revealed papilledema; rest of the neurological examination was
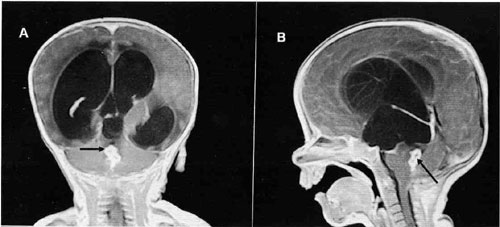
unremarkable. Chest X-ray was normal. MRI showed conglomerate ring
enhancing lesions in the fourth ventricle with moderate hydrocephalus (Fig.
1) and leptomeningeal enhancement in the left temporal region.
Surgical shunting of CSF was done by placing ventriculo-peritoneal shunt.
CSF examination of the patient demonstrated elevated protein levels (310
mg/dL) and low sugar (38 mg/dL) with 90% lymphocytes. CSF culture yielded
growth of Mycobacterium. Child was started on antituberculous treatment.
The patient was symptom free after three months and treatment was
continued for nine months.
 |
|
Fig.1 Contrast enhanced MRI images, (a)
coronal and (b) sagittal, showing conglomerate ring lesions (arrow)
in the fourth ventricle causing hydrocephalus. |
Common locations of intracranial tuberculoma are
cerebral and cerebellar hemispheres. Other less preferred locations being
quadrigeminal cistern, cerebellopontine angle and suprasellar region [1].
Extra-axial tuberculomas are rare and intraventri-cular lesions are even
less often seen [1-4]. This phenomenon is likely due to ventricles being
more immune towards various infections. The most likely route of
ventricular infections is through choroids plexus by hematogenous spread
[1]. In tuberculosis choroid plexus gets inflamed with formation of
tubercles, which may enlarge and form intraventricular tuberculoma.
Tuberculoma forma-tion in areas devoid of choroid plexus may be due to
formation of subependymal tubercles.
References
1. Desai K, Nadkarni T, Bhatjiwale M, Goel A.
Intraventricular tuberculoma. Neurol Med Chir (Tokyo). 2002;42:501-3.
2. Sonmez G, Ozturk E, Mutlu H, Sildiroglu O, Haholu A,
Kutlu A, et al. An unusual intraventricular lesion: tuberculoma. J
Neuroradiol. 2008;35:63-4.
3. Khanna PC, Godinho S, Patkar DP, Pungavkar SA,
Lawande MA. MR spectroscopy-aided differentiation: "giant" extra-axial
tuberculoma masquerading as meningioma. Am J Neuroradiol. 2006;27:1438-40.
4. Vajramani GV, Devi BI, Hegde T, Santosh V, Khanna N,
Vasudev MK. Intraventricular tuberculous abscess: a case report. Neurol
India. 1999;47:327-9.


