|
|
Lead Article Indian Pediatrics 2007; 44:91-100 |
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
Low dose ‘Sprinkles’ - An innovative Approach to Treat Iron Deficiency Anemia in Infants and Young Children |
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
Iron deficiency anemia (IDA) is one of the commonest nutritional disorders in children worldwide. Various studies in India have reported the prevalence of anemia in infants and children varying from 60% to 80%(1-5). Nutritional anemia is usually a result of inadequate iron stores at birth, poor weaning practices and recurrent infections and often goes unnoticed with adverse consequences on physical and mental development(6). The 1990 World Summit for Children, WHO, UNICEF(7,8) and more recently the Copenhagen Consensus(9) ranked micro-nutrient supplementation the second highest priority in advancing the lives of people in developing countries. The National Program for prophylaxis of IDA in India provides 100 pediatric tablets of iron (20 mg elemental iron as ferrous sulfate) for distribution to infants and children. The practical difficulties of administering tablets to babies has led to a virtual failure of this scheme(10,11). Alternate strategies for iron supplementation are now being explored. Iron ‘drops’ and syrups are used extensively in clinical practice, but are probably unsuitable for community use as they have to be carefully measured before use, have a metallic unpleasant taste, stain the teeth and require additional glass bottles for dispensing(12). ‘Sprinkles’ is a novel form of microencapsulated iron, which can be packaged in easy to use sachets for fortifying infants’ weaning foods at home(13-14). For a community setting, UNICEF recommends a daily dose of 12.5 mg of iron (as ferrous sulfate drops) for children 6-24 months old(15). However, the absolute amount of absorbed iron varies with the dose of iron, the form of iron compounds and different modes of delivery (drops, tablets, iron-fortified foods). This study was therefore designed to evaluate the efficacy of varying doses and forms of iron in Sprinkles on the hematologic status of children in a community setting in India. Subjects and Methods Study area The study was conducted between September 2004 and August 2005 in the Vadu Rural Health Program of the KEM Hospital that covers a rural population of 67,000 in 22 villages of Pune District, the State of Maharashtra. The study area is known to be chronically drought prone and is now experiencing improved socio economic development through industrialization, irrigation and communication facilities. The Vadu Rural Health Program of KEM Hospital, Pune provides primary and secondary health care services to the population through a 35-bed rural hospital at Vadu Budruk village and its network of sub-centers, mobile clinics and field based health workers. The area is not malaria endemic with only sporadic cases being reported annually. Design The study was designed as a double-blinded Cluster Randomized Community-based Trial. We listed all villages on chits of paper and blindly drew lots without replacement from an opaque bag to randomize the 22 villages into 5 groups. Four of the five groups were randomly assigned to receive identical looking Sprinkles™ sachets containing different dosages of elemental iron. Of the four Sprinkles groups, three provided iron as microencapsulated ferrous fumarate (Descote Ferrous Fumarate 60, Particle Dynamics Inc.), at doses of 12.5 mg (FF12.5), 20 mg (FF20) or 30 mg (FF30) and one provided iron as micronized ferric pyrophosphate (SunActive Fe™, Taiyo International) at a dose of 20 mg (MFP20). Sprinkles sachets additionally included ascorbic acid (30 mg), vitamin A acetate (300 mcg), Folic acid (160 mcg) and Zinc gluconate (5 mg). The fifth group (DROPS) received 20 mg elemental iron in the form of ferrous glycine sulfate drops (Fersoft™, MagnaChem). From our Surveillance Database we identified and screened all children from these villages for eligibility criteria: (i) age between 6 to 18 mo, (ii) taking semi-solid or solid weaning foods, (iii) currently not taking any hematinic, (iv) likely to remain in the study area for the next 2 mo, and (v) absence of any major illness, severe malnourishment (WAZ scores <3 of NCHS reference standard) and disability. Hemoglobin was determined using Hemocue™ hemoglobin photometer (Hemocue, Angelholm, Sweden). Only those children with hemoglobin between 70 and 100 g/L were enrolled after obtaining written parental consent. Severely anemic children (Hb <70 g/L) were excluded from the trial and referred to Vadu Hospital or KEM Hospital for further management. Monitoring Caregivers were instructed to add the contents of the Sprinkles sachet to a small portion of the child’s meal serving (after it was cooked) once daily for a 2-month period at any mealtime. Those in the DROPS group were instructed to give a measured dose of 1.5 mL (equivalent to 20 mg elemental iron) once daily for a 2-month period. Our field investigators paid a weekly visit for the next 2 months to monitor consumption of Sprinkles or Drops and recorded side effects, concurrent illness, ease of use and whether the child appeared to like either Sprinkles or Drops. These house visits also served to motivate caregivers to give Sprinkles or Drops. Data collection At enrolment, information was collected on socio-demographic characteristics of the house-holds including the Standard of Living Index (SLI) and the child was weighed using Salter type spring balance and supine length measured with an Infantometer. Hemoglobin was assessed on capillary blood by Hemocue™ at baseline, 3 and 8 weeks. In addition a venous blood sample was collected at baseline and 8 weeks for serum ferritin. These samples were transported within 4 hours to KEM Hospital, Pune in ice-lined vaccine carriers and serum separated by centrifugation within 6 h before storage at –40ºC. Serum ferritin was estimated using Monobind Inc, CA, USA ELISA kit. The sensitivity, intra and inter assay coefficient of variation were 1.0 ng/mL, 5.0% and 7.2% respectively. Information on side effects and concurrent illness was collected weekly including whether the child had experienced diarrhea, staining of the teeth, excessive crying, vomiting, and discoloration of stools, cough, cold or fever in the past seven days. The number of Sprinkles sachets or bottles of DROPS consumed was determined during weekly visits. Data processing Data was entered using a customized data entry package developed in Visual Basic and MS Access. The package was designed to minimize transcription and data entry errors with the aid of consistency checks and logical skips. Analysis runs were conducted independently by Indian research partners in STATA v8 and by the Canadian counterparts in SAS and compared. The primary outcome was hemoglobin at 3 and 8 weeks after the start of the intervention. Secondary outcomes included ferritin levels at 8 weeks, side effects, concurrent illnesses and compliance. Data on side effects and concurrent illness were analysed by determining the mean number of episodes per child (diarrhea, excessive crying, vomiting, cough, cold and fever) or whether a child had at least one reported incident over the 2 month period (teeth staining, stool discoloration). Compliance (expressed as mean percentage) was estimated as the total number of sachets consumed divided by 56, the total number expected to be consumed over the 8 weeks intervention period. Similarly, in the DROPS group, compliance measured as the number of bottles consumed by the study child divided by 6, the number of bottles expected to be consumed over the 8 weeks period. Statistical methods and sample size considerations Our sample size calculations were based on the primary outcome measure; change in hemoglobin levels. A total of 425 children (85 per intervention group) with a 20% drop out and a design effect of 2 for cluster randomization, had 90% power to detect a Hb difference of 10 g/L between groups, with an overall type I error of 5% (adjusted for multiple comparisons between the 5 groups using Bonferroni’s correction). Univariate descriptive analysis was used to compare baseline characteristics of children across the 5 intervention groups. For our primary outcome, we used paired Students’ t-test to compare change in Hb concentration from baseline to 8 weeks within groups and a Generalized Linear Model (GLM) to compare, between groups, the Hb concentration change from baseline to 3 and 8 weeks. Multiple comparisons of means between groups were computed using Tukey’s adjustment method. For our secondary outcomes, we used pair wise comparison of means using Tukey’s method to compare between groups, differences in compliance, side effects and other outcomes. All outcome variables were tested for normality. Serum ferritin was log transformed to attain normality. Lastly, we used multivariate analysis to explore the effects of Hb at baseline, mother’s education, compliance and other covariates on Hb change at 8 weeks. Ethical Approval The study was reviewed and monitored by independent Ethics Committees of KEM Hospital Research Center, Pune and Hospital for Sick Children, Toronto.
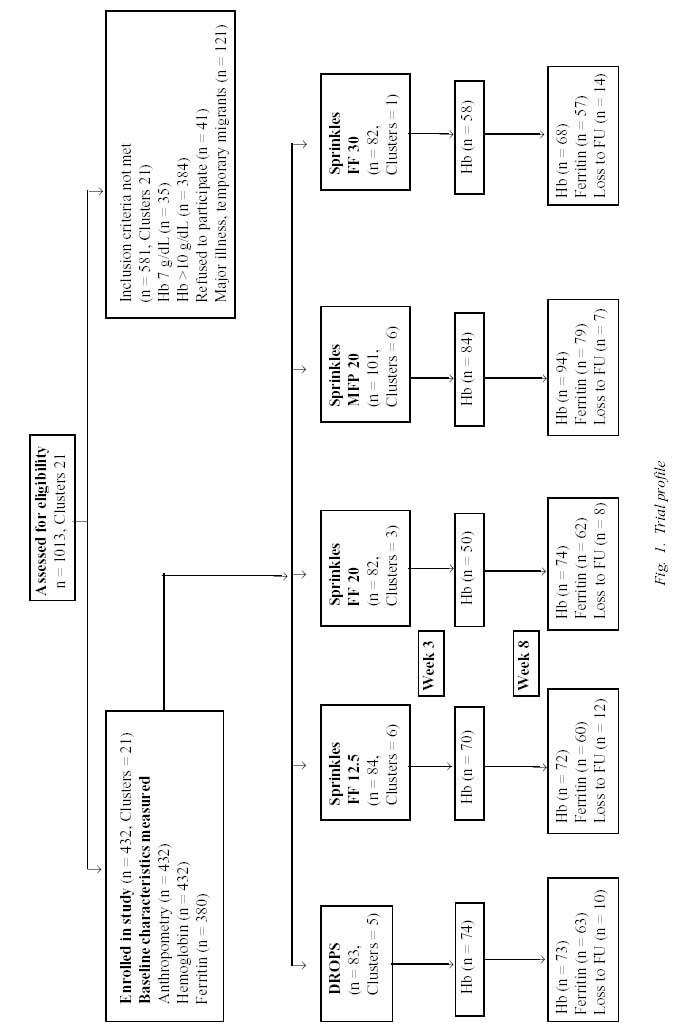
Results Recruitment (Fig. 1) Of a total of 1013 children (clusters = 21) assessed for eligibility, 432 children entered the study after excluding 41 refusals, 35 severely anemic children (<70 g/L), 384 children with normal hemoglobin levels (>100 g/dL) and 121 children for other reasons such as major illness/disabilities, severe malnourishment and temporary migrants. Overall, loss to follow up was 12%. Refusal for venous blood collection at 8 weeks was the most common reason cited. Baseline characteristics (Table I) The overall prevalence of anemia (Hb <100 g/L) was 58%. Mean age of our study children was 11 months with no differences across groups. There were no significant differences in household and socio-demographic characteristics across groups. TABLE I Socio-demographic Household Characteristics
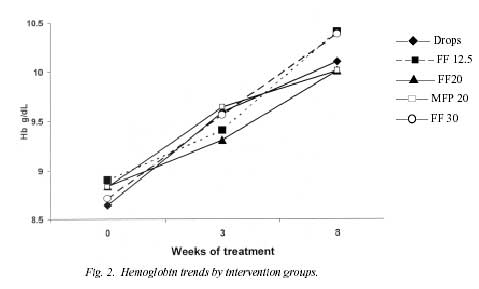
Ferros Glycine Sulfate; † Sprinkles - Ferrous Fumarate; ‡ Sprinkles - Sunactive Ferric Pyrophosphate* Effects on iron status (Table II) There was no difference in baseline Hb across groups (range 8.60 to 8.90 g/dL). There was a significant rise in Hb at 3 weeks (range 5.0 to 9.0 g/dL) and at 8 weeks (range 12.9 to 16.6 g/dL) in all groups with no significant differences across groups. Fig 2 shows the change in Hb levels from baseline to 3 and 8 weeks of intervention. Similarly, there was a significant decrease in the proportion anemic in each group with no differences across groups. Ferritin levels at baseline were similar across groups (range of median from 2.5 to 4.6 ng/mL). Ferritin levels showed a significant increase at 8 weeks from baseline within each group with no differences across groups. TABLE II Baseline to 8 Weeks Comparison by Group
Hemoglobin g/dL: mean (SD); * adjusted for baseline Hb; † Hb <10 g/dL; ‡ Serum ferritin: median, (range); § p value for log transformed ferritin change from baseline to 8 wk; ** p value for log transformed ferritin; †† p value for log transformed ferritin adjusted for baseline log ferritin.++
Compliance, side effects and concurrent illnesses (Table III) Median compliance varied across the groups (46%-62%). Compliance was significantly lower in the Sprinkles FF 30mg and the DROPS group as compared to the other Sprinkles groups (p value = 0.000). Pair-wise comparisons revealed that diarrhea, vomiting and staining of teeth were significantly higher with DROPS compared to Sprinkles. Stool discoloration was significantly more common with DROPS and Sprinkles FF 20 mg compared to other groups. A dose dependent relationship was not seen with side effects. Across all groups, almost all caregivers reported that children liked Sprinkles and DROPS and reported that they were easy to administer. Common cold, cough and fever were significantly more common amongst the DROPS group compared to all Sprinkles groups. TABLE III Side effects, Acceptability and Concurrent Illness Comparison Across Groups
10 Mean episodes per child over 2 mo follow up period. 11 Proportion children who reportecd the side effect at least once in the 2 mo follow up period. A multivariate analysis using Generalized Linear Modeling showed Hb increase at 8 weeks to be inversely related to Hb at baseline, and directly related to compliance and weight of the child after adjusting for age, sex, length of the child, iron status (ferritin) at baseline, socio-economic status and the intervention group. There were two deaths in our study. Both deaths were investigated by a Clinician using standardized and validated verbal autopsy to ascertain cause of death. One was a 14 mo male child (FF 30 mg group) who died one month after completion of 8 weeks of iron supplementation. Cause of Death was ascertained to be Infective Gastroenteritis and dehydration. There were no episodes of diarrhea or vomiting in this child during the iron supplementation period. The second was a 14 mo female child (MFP 20 mg group) who had a sudden death during the 7th week of iron supplementation. The child had self-limiting episodes of diarrhea / vomiting in the 1st 3rd and 6th week of iron supplementation. On the day of death, while playing, she had sudden onset crying, refused feeds followed by frothing at mouth and listlessness. The child died on way to hospital. The probable cause of death was given as meningitis or aspiration following a febrile convulsion. Both deaths appeared to be unrelated directly or indirectly, to Sprinkles, and the Ethics Review Committees from Canada and India permitted continuation of the trial. Discussion The ideal dose of iron supplementation for prophylaxis of IDA in community programs has long been an issue of debate. This double-blind cluster randomized clinical trial was conducted in a community setting to evaluate the hematological responses to various doses and forms of iron using Sprinkles versus traditional iron drops. We used iron drops (ferrous glycine sulphate) in a dose equivalent to 20 mg of elemental iron to match the dose recommended by the National Program for Control and Prevention of Anemia(16). Since Sprinkles is to be mixed with food, the absorption of iron in Sprinkles may be affected by the phytate content of the weaning foods. On the other hand, it is known that in the presence of iron deficiency, higher amounts of iron from Sprinkles are absorbed even with food(14,17). Hence, to determine the lowest efficacious dose of iron in Sprinkles, we evaluated 3 doses of iron (ferrous fumarate) in Sprinkles viz., 30 mg, 20 mg and 12.5 mg. We also included a trial arm of micronized ferric pyrophosphate ‘SunActive’ form of Sprinkles in a dose of 20 mg. Our study found a significant increase in hemoglobin levels as early as 3 and 8 weeks from baseline in all the groups with no differences across groups. Similarly, ferritin levels increased significantly in all groups (with no differences across groups). The number of children with anemia also decreased significantly in all intervention groups. Therefore, we conclude that Sprinkles containing 12.5 mg of ferrous fumarate are as efficacious as higher doses of Sprinkles or iron drops in raising hemoglobin levels in children. Diarrhea, vomiting, staining of teeth and discoloration of stools were all significantly higher in the iron drops group when compared with Sprinkles. Side effects, however, were similar within the Sprinkles groups and unlike previous studies(11) using iron drops as a supplement we did not find any dose-dependent relationship of Sprinkles with side effects. Most side effects were benign and were managed with reassurance and occasionally with symptomatic therapy. Although there was some reporting of teeth staining using Sprinkles, this may have resulted from an inadequate understanding that Sprinkles cannot be mixed with hot foods which may have caused the melting of the lipid coating the iron. Adherence to intervention i.e., ‘compliance’ was lowest in drops and poor in Sprinkles 30 mg as compared to the other Sprinkles groups. This may have been a result of the higher reporting of side effects and morbidity in these groups. However, our study shows overall lower compliance across all groups (group range 46% to 62%) as compared to other Sprinkles studies (7% to 85%). This is possibly because parents of our study children often stopped iron during concurrent illnesses like diarrhea, fever or respiratory illnesses (which are known to be frequent in this age group). However, almost all parents reported that Sprinkles (as well as drops) were easy to use and pleasant in taste. The results of this study are comparable to previous studies examining the hematologic effect of Sprinkles(18,19) and other studies using more traditional forms of iron supplements(20,21). As in other iron absorption studies using various doses and forms of iron added to cereals, rise in hemoglobin was higher in iron deficient children(22,23). Lower doses of iron, if effective, are to be preferred in community settings where individualized screening and monitoring of side effects may not be possible. The study findings need to be viewed within some contextual limitations. It was a controlled dose ‘efficacy’ trial and should not be viewed as an ‘effectiveness’ study. Our findings are limited to moderately anemic children (Hb 7-10 g/dL), though it is possible that the beneficial effect seen in anemic children will also be seen in preventing anemia in non-anemic children. Another limitation was that we did not include in-depth interviews and focus group discussions to ascertain a more detailed assessment of the advantages and disadvantages associated with the use of Sprinkles. These techniques may have enabled a better understanding of the acceptability of Sprinkles within the community. The advantage of ‘Sunactive’ micronized Ferric Pyrophosphate is that it mixes well with liquids or solids as against regular ‘Sprinkles’ which cannot be given in liquids. However the effect of this advantage was not included in our study as SunActive powders are still too expensive to be used in community program settings. As in many community based clinical trials we faced a number of methodological problems. Some of the study areas became inaccessible during the Monsoons. An epidemic of viral diarrhea led to wide spread though temporary stoppage of the iron interventions. Though capillary puncture for hemoglobin estimation by Hemocue was well accepted, venous blood sampling of babies for other hematology indices was resented by many parents. Two deaths in the study children (unrelated to Sprinkles) led to misgivings within the community. These and other problems created difficulties with compliance and delays in study ‘timelines’. Despite these difficulties, anemia was cured in over 60% of study children within a period of 2 months. In summary, our study suggests that iron in the form of Sprinkles is well absorbed when given with food and a dose as low as 12.5 mg in Sprinkles for 2 months is effective in improving the hematological profile of anemic children. Large scale ‘pilot’ studies are now needed to test the effectiveness of Sprinkles in treatment and prevention of anemia in children before they are scaled-up to community health programs. Acknowledgement The study was possible through a research grant from the Canadian Institutes for Health Research. The authors acknowledge the support of Heinz India in facilitating the procurement of Sprinkles. Heinz India has had no role in conceptual or design or any other phase of the study. Thanks are due to Dr. Padbidri, Director Research, KEM Hospital Research Center for his technical and administrative guidance. Thanks are due to Dr. Sheetal Salvi, Pallavi Marathe and Trupti Yadav for data management. The authors thank the Surveillance team led by Dr. Sanjay Juvekar of the Vadu Rural Health Program for their support in follow up. Lastly the authors are grateful to the children and their parents who consented to participate in the study. Contributors: SZ, AP and CS conceived and designed the study. SH, SB, AC and ZH were responsible for the design and management of the study. SN was responsible for biochemistry and relevant quality control. SH, AB and AC carried out the analysis. All authors contributed to the review and approval of the manuscript. Work supported by grants from: Canadian Institute for Health Research Competing interests: SZ owns the intellectual property rights to micronutrient Sprinkles™. The HJ Heinz Company is supporting the technical development of Sprinkles on a cost-recovery basis. Any profits from administrative fees on the technology transfer of Sprinkles is currently donated to the Hospital for Sick Children Foundation. There are no other ‘competing interests’.
| ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
References | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
![]()