|
|
Case Reports Indian Pediatrics 2007;44:138-140 |
||
|
Recurrent Acute Disseminated Encephalomyelitis |
||
|
Deepa Divekar
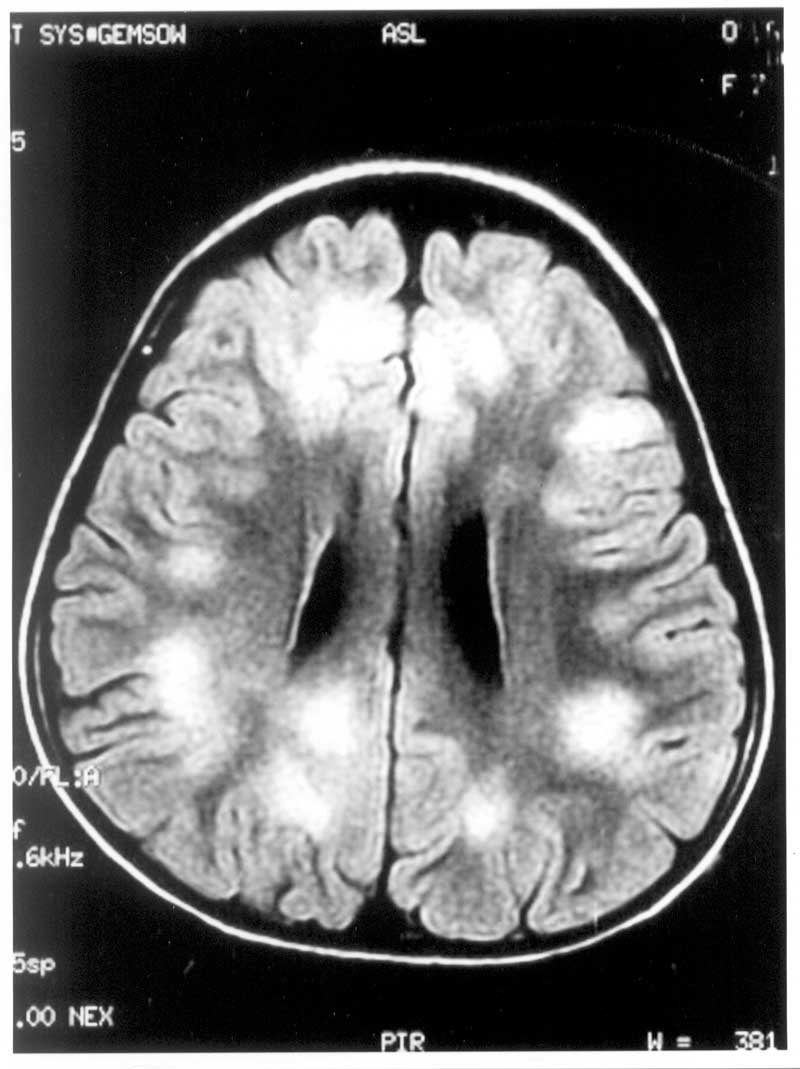
Abstract: Acute disseminated encephalomyelitis (ADEM) is an inflammatory demyelinating condition, which is usually monophasic. Recurrent ADEM is a much less characterized entity and its differentiation from multiple sclerosis (MS) poses a diagnostic challenge. We report a seven year old girl with recurrence of ADEM after 19 months and discuss the diagnostic issues involved. Key words: Demylenation, Encephalomyelitis. ADEM, a non-vasculitic inflammatory demyelinating condition, usually follows a monophasic course. Recurrent ADEM is a much less characterized entity and its differentiation from multiple sclerosis (MS) is a diagnostic challenge(1). The distinction between these two entities is important because ADEM has good long-term prognosis over MS(2). We present a case of recurrence of ADEM after 19 months of disease-free interval and review the diagnostic issues involved. Case Report A 7-year-old girl presented in April 2004 with fever, cough, headache, fatigue and vague bodyache of 2 to 3 days duration followed by progressively increasing drowsiness. There was no history of seizures, rash or recent vaccination. The sensorium was altered (GCS 13/15); cranial nerve examination was normal and there were no focal motor or sensory signs. Deep tendon reflexes were depressed with bilateral extensor planter response. There were no meningeal signs. The systemic examination was unremarkable. Blood counts and biochemical parameters were within normal range. Her cerebrospinal fluid (CSF) profile was normal with 2 WBCs, proteins 15 mg% and sugar 85 mg%. MRI brain revealed hyperintense signals on T2 and FLAIR sequences over bilateral subcortical white matter and cerebral cortices; they also involved basal ganglia, pons, midbrain, thalami, cerebellar peduncles and cerebellar white matter (Fig. 1). The corpus callosum was spared. She was treated with intravenous methyl prednisolone for 5 days. She had complete neurological recovery within a week. Her follow-up MRI done four months later showed complete disappearance of the abnormalities seen in the first MRI.
She presented after 19 months (November 2005) with similar viral prodrome of fever, cough, malaise and occasional vomiting. This was followed by altered sensorium and decreased limb movements of right side 8 days later. There was no history of seizures, rash or recent vaccination. Her neuro-logical examination revealed altered sensorium with Glasgow Coma Scale of 9/15, left gaze palsy, right hemiparesis, bilateral brisk deep tendon reflexes and extensor plantar response. The papillary response and fundi were normal. There were no meningeal signs. Other systems revealed no abnormality. Her hemogram showed WBC count of 18,000 with 85% polymorphs. The CSF was normal. MRI brain revealed hyperintense lesions on T2 and FLAIR at the same location as were observed in the first episode. She was investigated for causes of recurrent encephalopathy. Her CSF and blood lactate levels were normal as was urine and plasma amino-acidgram. Her tests for autoimmune diseases (LE cell, RA factor, ANA, dsDNA and lupus anticoagulant) were negative. Serological tests for the presence of HSV 1 & 2 and Japanese B in CSF yielded negative results. Her CSF was negative for oligoclonal bands. She was diagnosed as having recurrence of ADEM and was treated with intravenous methylprednisolone for 5 days followed by oral steroids for 3 weeks. She had complete neurological recovery within two weeks. Her follow-up MRI three months later showed significant reduction in the number and size of the lesions. Discussion The clinical features in our case were indicative of recurrent encephalitis with extensive lesions involving subcortical white matter, cerebral cortex, basal ganglia, midbrain, pons, cerebellum and thalami. The characteristic features of this case were the reappearance of symptoms and the lesions in the MRI that were at the same location after 19 months of interval with normal imaging in between. Such recurrent CNS symptoms raise the possibilities of MS or systemic disease with CNS involvement such as collagen vascular disease. Our case neither had any systemic features nor autoantibodies that suggested collagen vascular disease. MS becomes the second differential to ADEM and at times it is difficult to distinguish these two diseases, particularly in relapsing cases. From their retrospective study, Hynson and colleagues(3) had concluded that viral prodrome, ataxia, involvement of deep nuclei and absence of CSF oligoclonal bands are more indicative of ADEM than MS. Brass, et al.(4) are also of the opinion that presence of systemic and nonfocal neurological signs (fever, fatigue, headache, vomiting, encephalopathy) favored the diagnosis of ADEM over MS. Dale, et al.(5) described that polysymptomatic presentation; pyramidal signs, encephalopathy, bilateral optic neuritis and blood leucocytosis are more commonly observed in ADEM. The MRI findings that strongly suggest ADEM over MS are bilateral, asymmetric, involvement of cerebral white matter along with involvement of basal ganglia, thalamus, cerebellum and sparing of corpus callosum and periventricular region(6). However, the confusion between recurrent ADEM and MS still persists despite various published reports on recurrent ADEM illustrating character-istic MRI findings(7). Cohen, et al.(1) have studied the features of five cases of recurrent ADEM, this being the largest case series of recurrent ADEM reported so far. They have reported that in recurrent ADEM, the involved territories tend to be the same as that affected before and neuropsychiatric features are common during relapse. Our case also had same territorial involvement during the relapse; however she did not have any neuropsychiatric features at relapse. Contributors: DD Consultant in-charge, Conception and design of study, Critical revision of manuscript, SB Involved in patient management, Acquisition of data, Drafting of manuscript and PD Analysis and interpretation of data, Critical revision of manuscript. Funding: None. Competing interests: None.
| ||
|
References | ||
|
![]()