|
|
Brief Reports Indian Pediatrics 2001; 38: 169-173 |
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
Evolution of Otogenic Brain Abscess and Management Protocol |
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
Manuscript received: January 21, 2000; Despite widespread use of antibiotics, brain abscess following chronic suppurative otitis media (CSOM) remains a major problem for the pediatrician, neurologist, otologist and neurosurgeon. Brain abscesses constitute about 8% of all intracranial lesions(1). Otogenic brain abscess may constitute about 70% of brain abscess(2). Middle ear suppurative disease may extend to temporal lobe or cerebellum via various routes. Intracranial abscess follows a typical evolution in its formation(3) and its management differs at various stages of its formation(4). In this communication, we report our experience with otogenic brain abscess.
We conducted a retrospective analysis of 68 cases of otogenic brain abscess in children treated at various stages of their evolution in the Department of Neurosurgery, G.B. Pant Hospital, New Delhi during the last 9 years. All these cases were referred as chronic suppurative otitis media (SOM) (non cholestea-toma stage). There was no case of acute otitis media with abscess formation. The duration of CSOM varied from 6 weeks to 12 months. A majority of these cases were referred from elsewhere after diagnosis with a CT scan. Headache, vomiting and fever were among the most common symptoms. Some children had repeated convulsions, neurological deficit or altered sensorium (Table I).
The study population was divided into 3 groups based on the CT scan findings of evolution of abscess formation: (i) Group I – Stage of early cerebritis; (ii) Group II – Stage of late cerebritis; and (iii) Group III – Stage of capsule formation. Both Groups I and II were managed on conservative treatment. However, Group III required surgical drainage using twist drill aspiration or excision along with antibiotics. Surgical aspiration was done under local anesthesia. Pus which could be aspirated freely was taken out. After aspiration, the abscess cavity was instilled with 4-8 mg of Inj. gentamicin. Aspiration was repeated on the third and seventh day. Bacteriological result on the pus from the ear was not available in most of the cases. However, intracranial pus was routinely sent for aerobic culture and sensitivity. Antibiotics were selected according to sensitivity report and were given for 8-12 weeks. Injectable antibiotics were initially given for two to three weeks followed by oral antibiotics for three to eight weeks. Anticonvulsants were recomm-ended to all the patients of supratentorial abscess. Steroids were not used in any case after the diagnosis was confirmed on CT scan. Mannitol was used in two unconscious patients and in one with altered sensorium. CT scan was repeated on seventh day and 6 weeks after surgical intervention as per departmental protocol. All patients were referred to ENT surgeon for mastoidectomy subsequently.
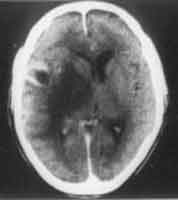
There were 50 boys and 18 girls with age ranging from 7 months to 13 years. There were 58 temporal and 10 cerebellar abscesses. Sixty six patients had unilocular and 2 had multiocular abscesses. Group 1: There were 8 patients in this group where the CT scan showed features of early cerebritis only (Fig. 1). This group was managed successfully with antibiotics alone. These patients were treated either with crystalline penicillin and chloromycetin and metronidazole; or cefotaxime and gentamicin and metroindazole depending upon availability and socioeconomic status of the patients.
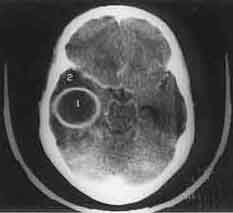
Group II: This group consisted of 12 patients with CT findings of late cerebritis (Fig. 2). Ten patients were cured on the same antibiotic protocol as in Group I. Only 2 patients further progressed to stage of capsule formation (Fig. 3) inspite of antibiotic cover. These two responded to twist drill aspiration.
Group III: A majority of patients referred to us (n = 48) belonged to this group. They were managed surgically by twist drill aspiration. Four patients responded to single tapping. Forty patients required 3 tappings at an interval of 3 to 10 days each before any radiologically significant reduction or disappearance of abscess was documented. Only 4 cases required surgical excision of the abscess. In 38 cases, the pus was sterile on culture and sensitivity. In the remaining, culture showed growth of Staph. aureus (n = 1), Strept. viridans (n = 2), E. coli (n = 1), Proteus (n = 1) and mixed infections (n = 5). Surgical excision of abscess was required under general anesthesia in 4 patients. Two patients had multilocular abscess, and other two had not responded to repeated tappings. Clinical improvement was 100% in Group I. Ten patients of Group II improved with antibiotics. Clinical improvement was seen in 40 patients in Group III who were treated with twist drill aspiration. However, 4 cases had residual neurological deficit (two hemiparesis, one optic atrophy and one cerebellar signs). Three of the four patients who underwent surgical excision showed complete neuro-logical recovery. There were two deaths, both in Group III, due to very poor general condition of the patients at the time of their referrals (GCS less than 6). Both these patients had large abscesses of more than 5 cm size. One was located in the cerebellum and another in the temporal lobe. Both had associated hydrocephalus and mass effect.
CT Scan has dramatically increased the pickup rate of intracranial abscess even at the early stage of its formation. It is now well established that selection of treatment modality depends on the stage of evolution of the abscess(4,5). Not all abscesses require surgical management. Based upon histopathological changes. Britt has described 4 stages of evolution of an abscess(3). In our experience it is more practical to subdivide abscesses into 3 distinct radiological stages only. These stages are based upon histopathological evolution of an abscess(5). CT scan shows a typical appear-ance at various stages. Stage-1: Stage of early cerebritis (Day 1-3). There is an ill-defined area of hypodensity on non contrast scan (NCCT). There is no evidence of capsule formation on contrast enhanced scan (CECT). This stage results from local inflammatory response indistinct from surrounding brain (Fig. 1). Stage II: Stage of late cerebritis (Day 4-9). CECT at this stage shows a thin ill-defined capsule. Pus formation begins here and is surrounded by a zone of inflammatory cells and macrophages. Edema is maximum at this stage (Fig. 2). Stage III: Stage of capsule formation (Day 10-14). NCCT shows smooth thin capsule, which shows a well-defined ring on giving contrast (Fig. 3). Capsule is usually thin on the medial side in the initial stages and as the evolution progress it becomes uniformly thick (Day 14 onwards). The fibroblasts and dense collagen are laid during this stage. Experimental and clinical evidence has confirmed that at least 15 days are required for encapsulation to occur(3,6). Britt had subdivided the stage of capsule formation into Stage III (early capsule forma-tion) and Stage IV (late capsule formation). Stage III shows diffusion of contrast into the abscess cavity in delayed infusion scan in 30-40 minutes whereas Stage IV does not reveal any diffusion of contrast material into the lucent center. There is further fading of contrast in delayed scan. In our experience infusion scans are not a routine practice. Hence, the distinction between early and late capsule formation does not really change the modality of treatment. There is no correlation between evolution of abscess and their clinical symptoms (Table I). In Stage I, most of the patients present with clinical features of meningitis. Similarly Stage II, presents with features of raised ICT, with a few patients (3 cases) having localizing sign and papilledema. Stage III, however presents with localizing sign, e.g., hemiparesis or features of herniation. The clinical symptoms of Stage II and Stage III may be overlapping; therefore, it is more relevant to differentiate radiologically between these two stages for proper treatment. Antibiotics are very effective in early and late cerebritis stages(4,7). The ineffectiveness of antibiotics in the stage of capsule formation is due to the acidic medium within the abscess cavity and the inability to have adequate therapeutic concentration of the antibiotic within the abscess(8). Therefore, surgical intervention is essential once the capsule is well formed(2,4,9). Surgical intervention can be either by repeated tappings or excision. It is, therefore, very essential to diagnose an abscess at an early stage of its evolution, as it avoids surgical intervention. Steroids reduce brain edema but diminish the effectiveness of the host defense mechanisms that assist in containment of infection. Steroids inhibit collagen capsule formation and also inhibit migration of leucocytes. They are therefore, avoided in the stages of early and late cerebritis(10). There can be various modes of surgical management. Stereotactic aspiration(11) and endoscopic drainage(12) are some of the newer modalities. Burr hole aspiration is still used with 2.7% mortality(2). In our series, drainage was successfully done without making any burr hole in the skull. A 2-3 mm drill is as effective as a burr hole in draining the pus. This can even be done under local anesthesia at the bedside. In conclusion, brain abscess following CSOM can be effectively managed if the evolution pattern is known, as the treatment is now mainly based on the stage of abscess formation. Contributors: DS participated in drafting the paper, AKS, DS and SS contributed their cases for analyses, and will act as guarantors for the paper. VG helped in internet search and review of literature.
Funding:
None.
| ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
![]()