|
|
|
Indian Pediatr 2015;52:
1047-1050 |
 |
Renalase Levels in Children with Solitary
Functioning Kidney
|
|
K Taranta-Janusz, R Roszkowska and A Wasilewska
From Department of Pediatrics and Nephrology, Medical
University of Bialystok, Poland.
Correspondence to: Dr Katarzyna Taranta-Janusz,
Medical University of Bialystok, Department of Pediatrics and
Nephrology, 15-274 Bialystok, Waszyngtona 17, Poland.
Email: [email protected]
Received: December 24, 2014;
Initial review: February 25, 2015;
Accepted: September 19, 2015.
|
Objective: To measure serum and urine renalase levels in children
with a single kidney, and to compare with a reference group.
Methods: Participants were: solitary kidney (n=36)
and healthy children (n=57). Renalase levels were measured using
the immunoenzymatic method.
Results: Serum and urine renalase levels were
significantly lower in patients with a solitary kidney compared to
healthy children. Urine renalase/creatinine values were negatively
related to serum creatinine and positively related to glomerular
filtration rate. Significant correlations between renalase levels and
blood pressure were not found.
Conclusions: Prognostic importance of reduced
renalase levels in children with a single kidney can only be quantified
by further longitudinal study.
Keywords: Chronic kidney disease, Nephrectomy, Solitary
functioning kidney
|
|
T
he long-term outlook for patients born with a
single kidney or following unilateral nephrectomy in childhood is
controversial. Animal studies suggest that the resultant compensatory
increase in single nephron glomerular filtration rate may lead to
progressive damage of the remaining renal tissue leading to hypertension
[1]. Low nephron number is reported to be associated with hypertension
and chronic kidney disease in humans [2,3].
Xu, et al. [4] described a novel substance
called renalase, and its possible role in the pathogenesis of
cardiovascular complications. Renalase is a monoamine oxidase of renal
origin responsible for the degradation of catecholamines. Renalase
lowers blood pressure by decreasing cardiac contractility and heart rate
and by preventing the expected compensatory increase in peripheral
vascular tone. Abnormalities in the renalase pathway are described in
animal models of hypertension and chronic kidney disease [5].
This study was performed to measure serum and urine
renalase levels in children with a solitary functioning kidney, and
compare these with healthy children.
Methods
Inclusion criteria for cases were: age <18 years, and
a solitary functioning kidney (congenital or acquired) demonstrated by
ultrasonography and renal scintigraphy. Exclusion criteria were:
clinical and laboratory signs of infection, history of urinary tract
infection, use of medications that might influence renal function or any
kidney abnormalities detectable by ultrasonography. The reference group
was recruited from participants of the OLAF study [6], whose physical
examination, urine and blood tests, and renal ultrasonography were
normal. The study was approved by the Medical University Ethics
Committee.
Research methodology involved recording clinical
history, demographic data, and physical examination. Hypertension was
defined as blood pressure >95th percentile for age, sex, and height.
Venous peripheral blood after overnight fasting, and morning urine
samples were collected. Serum and urine samples were frozen and stored
at –80°C. Laboratory tests included: serum creatinine, urea, uric acid
and urinalysis. Glomerular filtration rate was assessed by an updated
Schwartz formula. Microalbuminuria was defined as urinary albumin/creatinine
ratio of 30-300 µg/mg.
Using a commercial enzyme-linked immunosorbent assay
kit (USCN Life Science Inc., China), serum and urine renalase levels
were measured and expressed as micrograms per milliliter (µg/mL) in the
serum, and nanograms per milliliter (ng/mL) in the urine. The intra- and
inter-assay coefficients of variance were 10% and 12%, respectively.
Detection range was 3.12-200 ng/mL.
The data were analyzed using Statistica 10.0 software
(StatSoft, Tulsa, OK, USA).
Results
The study cohort consisted of 93 participants divided
into: children with a single kidney (n=36). and reference groups
(n=57). Clinical and biochemical data of recruited patients are
summarized in Table I. Of 36 patients eligible for
analysis, 27 (75%) had a congenital and 9 (25%) had an acquired solitary
functioning kidney. The etiologies of the acquired single kidney were:
ureteropelvic junction obstruction (n=12), ureterovesical
junction obstruction (n=57), and reflux nephropathy (n=57).
Clinical and laboratory data of congenital single kidney patients did
not differ from those with acquired single kidneys. None of our single
kidney patients had proteinuria in morning samples; however, 4/36
patients (11%) were diagnosed with albuminuria. In the single kidney
group, 10 children (27.7%) were hypertensive. Glomerular filtration rate
<90 mL/min/1.73m 2 was found
in six patients.
TABLE I Clinical and Laboratory Data of the Children with Solitary Functioning Kidney and Reference Group
|
Solitary functioning kidney |
Reference |
P value |
|
median (IQR) (N=36) |
median (IQR) (N=57) |
|
|
Gender (M/F) |
23/13 |
35/22 |
|
|
Age (y) |
11.25 (6, 14) |
12 (7.5, 16) |
0.26 |
|
Weight (kg) |
37 (27.7, 60.5) |
37 (25.0, 58.6) |
0.94 |
|
Height (cm) |
145.7 (124.7, 163.5) |
143 (126.3, 169) |
0.49 |
|
Body mass index Z-score |
1.01 (–0.19, 1.79) |
0.28 (–0.26, 1.23) |
0.09 |
|
Serum creatinine (mg/dL) |
0.55 (0.46, 0.66) |
0.62 (0.49, 0.73) |
0.19 |
|
Glomerular filtration rate (mL/min/1.73 m2) |
107.38 (94.87 , 124.77) |
106.31 (97.11, 134.22) |
0.72 |
|
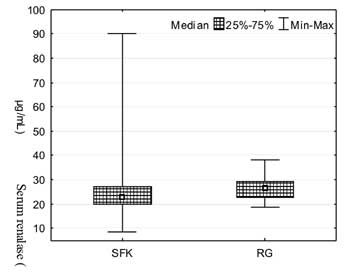
Serum renalase (µg/mL) |
23.07 (19.96, 27.22) |
26.75 (22.64, 29.20) |
0.04 |
|
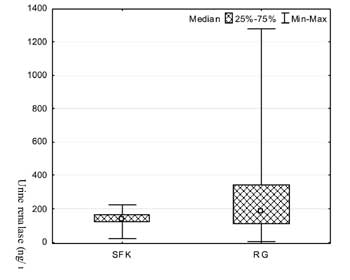
Urine renalase (ng/mL) |
145.28 (121.15, 163.33) |
187.93 (112.83, 342.25) |
0.01 |
|
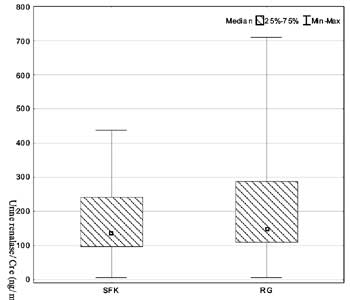
Urinary renalase-to-creatinine ratio (ng/mg) |
137.68 (96.05, 239.43) |
187.93 (110.45, 286.66) |
0.64 |
|
Kidney overgrowth (%) |
41.20 (20.25, 55.10) |
– |
– |
|
Urinary albumin-to-creatinine ratio (µg/mg) |
69.15 (37.68, 91.71) |
– |
– |
|
Systolic blood pressure (centile) |
71 (44, 89) |
58 (10, 63) |
0.44 |
|
Diastolic blood pressure (centile) |
60 (40, 73) |
49 (12, 72) |
0.47 |
Median serum and urine renalase levels were
significantly lower in single kidney patients when compared to the
reference group (P<0.05). Urinary renalase/creatinine levels were
comparable in both groups (Fig. 1).
Between the congenital and acquired single kidney
participants, or children with various etiologies of acquired solitary
functioning kidney, we found no differences in the serum and urine
renalase concentrations. Identical results were also obtained from
hypertensive and normotensive children.
We did not find significant correlation between
renalase levels and blood pressure. In the single kidney group, no
statistically significant difference was stand between the number of
children with decreased urine renalase/creatinine levels (<50th
centile) who were normotensive and hypertensive (P=0.71).
Reduction in urine renalase excretion was estimated according to
reference urine renalase values from the study of Rybi-Szumiñska, et
al. [7].
Serum renalase positively correlated with urine
renalase (r=0.35, P<0.05). The urine renalase/creatinine values
were negatively related to serum creatinine (r=-0.35; P<0.05),
and positively to glomerular filtration rate (r=0.37; P<0.05).
Kidney overgrowth did not correlate with serum and urinary renalase,
glomerular filtration rate, and urinary albumin/creatinine ratio.
ROC analyses were performed in order to define the
diagnostic efficiency of serum and urine renalase in identifying
children with renal dysfunction (glomerular filtration rate <90 mL/min/1.73m 2)
among patients with a solitary functioning kidney. In this analysis AUC
for serum (µg/mL) and urine renalase (ng/mL) did not reveal good
diagnostic accuracy in comparison to the urinary albumin/creatinine
ratio, and was 0.425, 0.587, and 0.985, respectively.
Discussion
Our study, designed to explore serum and urine
renalase levels and their relation to kidney function in children with a
single kidney, reported that serum and urine renalase levels were
significantly lower in single kidney patients. We did not find
significant differences in urine renalase/creatinine levels between
children with a solitary functioning kidney and the reference groups.
Moreover, urine renalase/creatinine values in single kidney patients was
related to parameters of kidney function: negatively with serum
creatinine and positively with glomerular filtration rate. Neither serum
nor urine renalase correlated with age, gender, or blood pressure.
The limitations of the study are: small sample size,
single center, and cross-sectional. Additionally, an appropriate
measurement of blood pressure in small children is difficult because of
"white coat" anxiety and poor cooperation. Furthermore, in prepubertal
and younger children no formula of glomerular filtration rate estimation
gives acceptable results.
Recent experimental data in animal models support the
hypothesis that renalase is an important marker of chronic kidney
disease [5]. In humans, several studies have examined the likelihood
that the presence of a solitary functioning kidney increases the risk of
hypertension, proteinuria, and renal failure during childhood [8]. It
has been shown that an apparently normal kidney is usually associated
with hypertrophy of the surviving nephrons and accompanied by renal
hyperfiltration which may contribute to albuminuria and a decline in
glomerular filtration rate.
Patients with chronic kidney disease demonstrate
markedly reduced levels of plasma renalase [9]. Based on our findings,
significant reductions in serum and urine renalase levels dependent on
kidney function were reported in single kidney patients compared with
healthy volunteers. Our finding of no significant relationships between
serum or urine renalase levels with age, gender, or blood pressure is in
agreement with studies in dialyzed adult patients [10].
Based upon these results, a decrease in renalase
levels may be related to early renal damage. However, these findings
should be interpreted with caution because data from our ROC analyses
did not show good diagnostic profiles for renalase in detection of renal
dysfunction.
We conclude that renalase levels are altered but are
unlikely to be suitable for the detection of early renal damage.
Prognostic importance of reduced levels of renalase in children with a
solitary functioning kidney to detect early deterioration of kidney
functions before hypertension develops should be quantified by further
longitudinal studies.
Contributors: KT-J: patient screening,
enrollment, outcome assesement, data analysis, writing manuscript; RR:
patient screening, data analysis, writing manuscript; AW: final data
analyses, writing manuscript, critical revision.
Funding: Supported by a grant from the
Medical University of Bialystok, Poland. Competing interests:
None stated.
|
What This Study Adds?
• Serum and urine renalase levels are
significantly lower in patients with a solitary functioning
kidney in comparison to healthy children.
• Prognostic importance of reduced levels of
renalase does not seem to be suitable for the detection of early
renal damage in children with solitary functioning kidney.
|
References
1. Hegde S, Coulthard MG. Renal agenesis and
unilateral nephrectomy: What are the risks of living with a single
kidney? Pediatr Nephrol. 2009;24:439-46.
2. Brenner BM, Garcia DL, Anderson S. Glomeruli and
blood pressure. Less of one, more the other? Am J Hypertens.
1988;1:335-47.
3. Hoy WE, Hughson MD, Bertram JF, Douglas-Denton R,
Amann K. Nephron number, hypertension, renal disease and renal failure.
J Am Soc Nephrol. 2005;16:2557-64.
4. Xu J, Li G, Wang P, Velazquez H, Yao X, Li Y,
et al. Renalase is a novel, soluble monoamine oxidase that regulates
cardiac function and blood pressure. J Clin Invest. 2005;115:1275-80.
5. Desir GV. Renalase deficiency in chronic kidney
disease, and its contribution to hypertension and cardiovascular
disease. Curr Opin Nephrol Hypertens. 2008;17:181-5.
6. Ku³aga Z, Litwin M, Grajda A, Ku³aga K, Gurzkowska
B, GóŸdŸ M, et al. OLAF Study Group. Oscillometric blood pressure
percentiles for Polish normal-weight school-aged children and
adolescents. J Hypertens. 2012;30:1942-54.
7. Rybi-Szumiñska A, Michaluk-Skutnik J,
Osipiuk-Rem¿a B, Kossakowska A, Wasilewska A. Normal values for urine
renalase excretion in children. Pediatr Nephrol. 2014;29:2191-5.
8. Westland R, Schreuder MF, Bökenkamp A,
Spreeuwenberg MD, van Wijk JA. Renal injury in children with a solitary
functioning kidney - the KIMONO study. Nephrol Dial Transplant.
2011;26:1533-41.
9. Desir GV. Regulation of blood pressure and
cardiovascular function by renalase. Kidney Int. 2009;76:366-70.
10. Zbroch E, Malyszko J, Malyszko J, Koc-Zorawska E,
Mysliwiec M. Renalase and catecholamines: causative factors or innocent
bystansers of hypertension in haemodialysis and peritoneal dialysis
patients. ERA-EDTA congress, Paris, May 24-27, 2012.
|
|
|
 |
|