|
|
Research Paper Indian Pediatrics 2007; 44:897-901 |
|||||||||||||||||||||||||
|
Subclinical Hypovitaminosis D Among Exclusively Breastfed Young Infants |
|||||||||||||||||||||||||
|
Resurgence of prolonged exclusive breastfeeding has led to a coincident increase in the incidence (28% 1990, 50% year 2000) of vitamin D deficiency in infancy(1). Exclusive breastfeeding, with inadequate vitamin D supplementation in the mother and baby, has been concluded to be the most important risk factor(2-4). Dark skin, low sunshine exposure, vegetarian diet, low intake of dairy products or vitamin D, predispose mothers and their breastfed infants to vitamin D deficiency(2-4). During pregnancy maternal vitamin D status influences the transplacental transfer of 25 hydroxy cholecalciferol (25(OH)D) to the fetus with a direct linear relationship between maternal and cord blood levels(3,5,6). As vitamin D content of human milk is low (15-50 IU/L) even in vitamin D replete mothers, transplacentally stored vitamin D, constitutes major source of vitamin D in early infancy in exclusively breastfed (EBF) infants(5-7). Optimal levels of 25 (OH) vitamin D in children and adults remain controversial. For optimal calcium and bone metabolism, 25 (OH)D levels in adults ranging from 15 to 20 to 31 ng/mL have been suggested(8,9). The Food and Nutrition Board, INS-USA, consider 25 (OH)D <15 ng/mL "low" and 15 to 25 ng/mL "low normal"(10,11). The objectives of this longitudinal study was to determine the vitamin D status of mother-newborn diads at birth and of their exclusively breast fed infants at 3 months. Subjects and Methods This was a longitudinal study done over a period of one year at a referral private hospital in western India. Enrollment criteria included healthy pregnant women, aged 20 to 35 years, weighing >45 kg, with a normal pregnancy resulting in the birth of term neonates weighing >2.5 kg. These mothers from middle income group were encouraged to exclusively breast feed their infants. The mother-infant diad were followed till 3 months and none of the infants received any mineral or vitamin supplementation. Only infants exclusively breast-fed at 3 months were included for the final analysis. Data collection Detailed maternal obstetric and medical details were recorded. Their daily dietary calcium and vitamin D intake was ascertained by dietician using a 3 day recall and supplements received were also recorded. Infant data such as weight at birth and 3 months, feeding history and mineral/vitamin supplementation history were recorded. Of the 42 mother/newborn diads included initially, 35 infants were available for follow up. Laboratory data: At 37 ± 1 weeks of gestation, maternal blood samples were taken for estimating serum calcium, phosphorus, heat labile fraction of alkaline phosphatase (HLAP) equivalent to bone alkaline phosphatase, and 25 (OH) vitamin D. The same biochemical parameters were estimated in cord blood and infants blood by 3 months (± 17 days). Serum was separated and divided into aliquots. Serum calcium, phosphorus and alkaline phosphatase were estimated by standard bio-chemical techniques on daily basis with adequate controls. Samples were stored at –70ºC for 25 (OH)D and estimated by Biosource RIA kit International (Netherlands). The kit values for 25 (OH)D ranged from 7.5 to 75 pg/mL. HLAP which constitutes 30% of total ALP was preferred as placental ALP raises the maternal and cord blood ALP. The levels for HLAP as mentioned on the kit were used as norms. In absence of specific norms for Indian infants, 25(OH) vitamin D <15 ng/mL was considered ‘low’, and 15 to 25 ng/mL as ‘low normal’(10,11). Data analysis and ethical approval: The means between groups was compared using student-t test. Correlation was determined using Pearson’s correlation coefficient. Institutional ethical approval was obtained for the study. Results There were 42 eligible mother-infant diads for final analysis. Maternal data: Nearly 80% were vegetarian with increased intake of dairy products during pregnancy. Daily dietary calcium intake ranged from 800 to 1500 mg besides the supplemental calcium (250- 500 mg) and vitamin D (125 – 400 IU) that they consumed. Supplements were discontinued by 33% women in the postnatal period. Table I shows the maternal serum values of calcium, phosphorus, HLAP and 25 (OH)D. In 37 (88%) mothers serum calcium was in normal range, while in 5 (12%) the values ranged from 7.1 to 7.7 mg/dL. In 21 (50%), the 25 (OH)D values were below 25 ng/mL (<15 ng/mL in 14, 15-25 ng/mL in 7). There was no significant correlation between maternal 25 (OH)D and calcium (r = –0.001), phosphorus (r = –0.173), or HLAP (r = 0.086). Table I Comparison of Mean (SD) Calcium, Phosphorus, HLAP and 25(OH)D levels in Mother, Cord Blood and Infants at 3 months
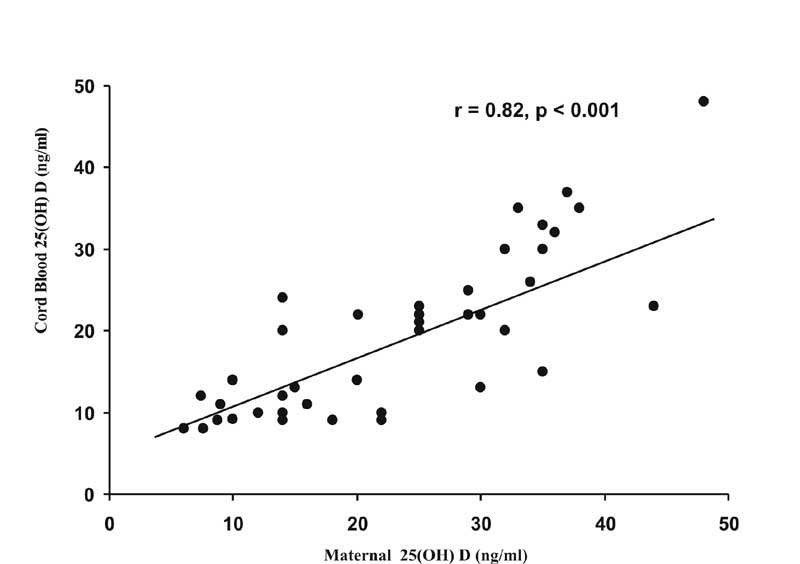
* Cord blood vs mother (p <0.01). # 3 month vs cord blood (p <0.05). Cord blood: The mean birth weight was 2.9 ± 0.38 kg and length was 48.5 ± 1.5 cm in the enrolled infants. The significantly higher (P <0.001) mean cord blood calcium and phosphorus (Table I) as compared to maternal values, indicate a positive transplacental gradient towards the fetus. Higher HLAP (P <0.01) probably reflected rapid fetal growth and skeletal metabolic activity. The mean cord blood 25 (OH)D was 19.36 ± 9.57 ng/mL. In 62% the levels were <25 ng/mL (<15ng/mL 36% , 15-25 ng/mL in 26%). There was a highly significant positive correlation (r = 0.82, P <0.001)(Fig. 1) between cord blood and maternal 25 (OH)D.
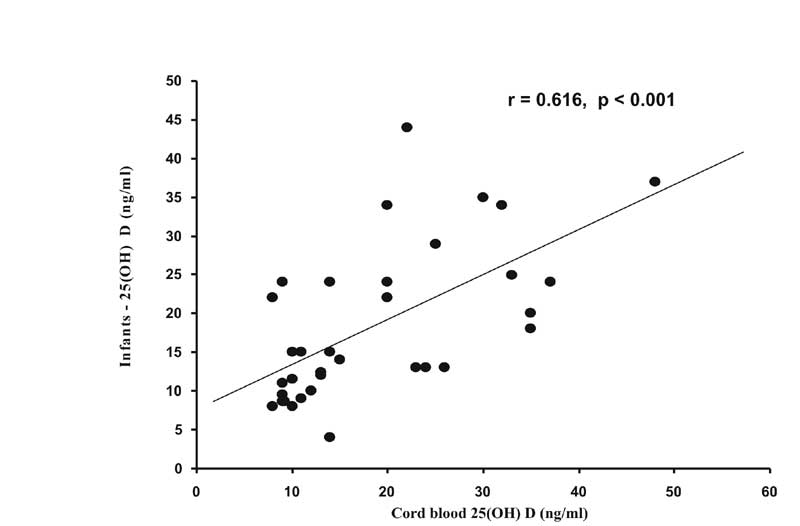
Three month infant data: At 3 months, 35 (85.3%) exclusively breast fed infants were available. Their mean weights and length were 5.6 ± 0.85 kg and 61.1 ± 3.16 cm respectively. Mean serum calcium at 3 months was significantly higher than at birth (P <0.05) (Table I). There were no differences in serum phosphorous and 25 (OH)D levels since birth. Though statistically not significant, 80% infants had 25 (OH)D <25 ng/mL, (<15 in 51%,15-25 in 29%) compared to 62% in cord blood. Higher 25 (OH)D at 3 months correlated with higher 25 (OH)D values in cord blood (r = +0.616, P <0.001, Fig.2) as well as higher antenatal maternal levels (r = + 0.552, P <0.001). This probably indicates the importance of prenatal maternal vitamin D status on infant vitamin D status. The significantly higher mean HLAP 306.7 ± 188.5 U/L compared to cord blood could not be correlated to abnormality of any other biochemical parameters [HLAP vs calcium (r = –0.179), phosphorus (r = –0.036), or 25 (OH)D (r = –0.038)]. In one (1/35) clinically normal infant with very low 25(OH)D, 4 ng/mL, Ca, P and HLAP (183U/L) were in normal range, suggesting inconsistent relationship between 25(OH)D and HLAP as reported (11). In 18 (51%) of these infants HLAP was above its median value of 287U/L, and in 15/18 (83%) of them the 25 (OH)D was <25 ng/mL. In the absence of PTH measurements, it was not possible to conclude whether this indicated bio-chemical hypovitaminosis D. Discussion Past few years have witnessed a revival of interest in the status of vitamin D nutrition at all ages. Several reports of nutritional rickets, hypo-calcemic seizures, subclinical / biochemical hypo-vitaminosis D in exclusively breast fed infants, have appeared from developed countries(2-7,11) as well as from countries with abundant sunshine as from middle East, Pakistan and Turkey(12,13). These have been attributed to sociocultural traditions and specifically to exclusive and prolonged breast- feeding without adequate supplementation of vitamin D in the mothers and their young infants. In the present study serum calcium levels were normal in nearly 90% mothers (total daily calcium intake of 1000 to 2000 mg), but mean 25 (OH)D (22.9 ± 10.9 ng/mL) was below 25 ng/mL in 50% (on vitamin D intake of 125 to 400 IU). In a recent Indian study on 207 pregnant women of lower socioeconomic group, the mean 25 (OHD) was 14 ± 9.3 ng/mL with very low values in 85%(14). The requirement of vitamin D during pregnancy and lactation is believed to be higher (upto 1000 IU) than currently recommended (DRI) 200-400 IU/day, which seems grossly inadequate(9). Significantly higher calcium and phosphorus levels in cord blood with good positive correlation with maternal 25 (OH)D levels, are a cardinal feature of foetal calcium, phosphorus and vitamin D metabolism(3,6,7), as also observed in this study. In the human fetus, vitamin D metabolism begins with 25 (OH)D, cord blood having 60% to 70% of maternal circulating 25 (OH)D(6,7,9). Optimal cord blood 25 (OH)D is not known(6,7,9). The mean cord blood 25 (OH)D (19.36 ± 9.57 ng/mL) was below 25 ng/mL in two-thirds of infants in the present study as compared to very low mean level, 8.4 ± 5.7 ng/mL (cut off used 20 ng/mL) in 102 newborns from Lucknow of lower economic group with levels <20 ng/mL in 96%(14). Two of the limitations of present study relate to small sample size and unavailability of PTH levels. However, data on precise threshold and level of 25 (OH)D when HLAP and PTH start rising is limited and variable (5,13). Very few longitudinal studies from birth to early infancy are available. On tracking these newborns at 3 months, they were clinically normal with significant increase (P <0.01) in calcium but no rise in 25 (OH)D. Though statistically not significant in this small study, 80% had suboptimal 25 (OH)D level <25 ng/mL versus 62% in cord blood. Also when maternal and hence cord blood 25 (OH)D levels were higher, the levels in infancy were maintained higher. A larger study on normal infants of higher economic group may help to determine optimal 25 (OH)D level in infancy and understand the relationship of biochemical hypovitaminosis D to the threshold values for rise in alkaline phos-phatase and PTH. Vitamin D insufficiency in pregnancy can limit fetal growth, limit the peak bone mass in adolescents and may contribute to involutional osteoporosis at a later age(3,4,15). Vitamin D supplementation for pregnant and lactating women in adequate doses, probably upto 1000 IU as suggested(3,9), for adequate length of time will also safeguard women’s health. The necessity for early vitamin D supplementation in exclusively breast-fed young infants should be based on prevailing circumstances in view of uncertain maternal vitamin D status. Acknowledgements The authors wish to thank all staff of Pediatrics, Obstetrics and Dietetics Departments of Sir H N Hospital & Research Center (HNHRC) and laboratory staff of Sir H N Medical Research Society (HNMRS) for their support, and Ms H Madav for secretarial help. We are also grateful to the Medical Director of Sir HNHRC for his kind permission to publish this work and to HNMRS for the financial grant for this study. Contributors: MPD, UB and PP conceptualized the project, MPD and UB designed it and UB collected and analysed the data and wrote the first draft of the study analysis. RM helped with the laboratory estimations and BC was the dietician and collected and analysed the data on diet. MPD and UB were involved in the preparation of the manuscript. MPD and PP are guarantors for the study. Funding: Sir H.N.Medical Research Society. Competing interests: None stated.
| |||||||||||||||||||||||||
|
References | |||||||||||||||||||||||||
|
|
![]()