|
|
Letters to the Editor Indian Pediatrics 2005; 42:1255-1256 |
|||
|
Unusual Congenital Cystic Adenomatoid Malformation of the Lung: A Diagnostic Dilemma |
|||
|
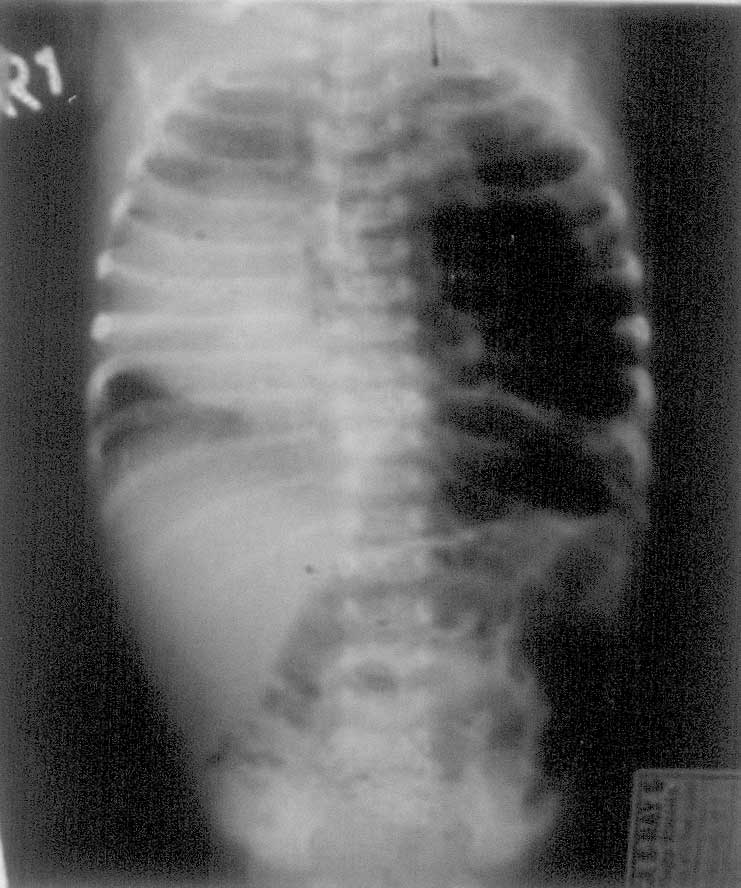
We report our experience with a neonate, aged 3 weeks, referred to us for progressively increasing respiratory distress since birth. No antenatal workup was available. The clinical and pre-operative radiological picture of the patient mimicked congenital diaphragmatic hernia (Fig. 1) for which he underwent laparotomy, which revealed normal abdominal anatomy with intact diaphragm. The follow-up chest radiograph showed hyper-inflated lung with mediastinal shift and was suggestive of congenital lobar emphysema. Keeping in mind the significant respiratory distress, a left thoracotomy was performed few hours later that revealed multiple cysts in left lower lobe of lung. Left lower lobectomy of lung was done. The histopathology of resected specimen however came as surprise; it was reported as CCAM. The child had stormy post-operative period. He required ventilatory and ionotropic support and succumbed to persistent pulmonary hypertension and sepsis on l0th post-operative day. CCAM has been known to mimic congenital diaphragmatic hernia, congenital lobar emphysema, bronchogenic cyst, and broncho-pulmonary sequestration, clinically as well as radiologically on chest roentgeno-gram(4). Hence, whenever the diagnosis is in doubt, a high resolution CT is advisable(5) helps in confirming the diagnosis, demonstrating unsuspected findings, with better depiction of anatomic extent of congenital lung anomalies, thus allowing better planning for surgery. However, we could not wait to get CT done as the neonate was deteriorating inspite of high-pressure ventilatory settings. Not being able to differentiate CCAM and CLE pre-operatively may not be very consequential, as both conditions need surgical excision but it is extremely important to differentiate CCAM from CDH as the two are managed differently. CCAM necessitates thoracotomy whereas CDH requires laparotomy after stabilization. CT scan can definitely resolve this diagnostic dilemma pre-operatively. Awareness of this entity and high degree of suspicion in cases of neonatal respiratory distress would improve our diagnostic accuracy and successful outcomes. Pathak, D.,
|
![]()