|
|
Case Reports Indian Pediatrics 2001; 38: 1421-1425 |
||
|
Acute Brucellosis of Childhood: A Case Report with Unusual Features |
||
|
Anil Sachdev Rakesh Vohra* Sunita Bijarnia
Bruecellosis is a zoonotic infection, transmitted to humans primarily by consumption of unpasteruized milk and milk products. The disease exists world wide especially in Mediterranean, Saudi Arabia, Latin America and Indian subcontinents(1). It is less often thought of in the differential diagnosis of a long standing fever and most of the time child is investigated for enteric fever and tuberculosis(2). Kadri et al.(3) reported 0.8% seropositivity among 3532 patients tested for brucellosis in Kashmir. We present a child of acute brucellosis with unusual clinical features, hematological and imaging findings. Case Report A 6-year-old male child of Indian origin, resident of New Delhi, was admitted in October 1999 with complaints of fever and dry cough for 5 days, headache and three episodes of nonbilious vomiting for 1 day. He also had two episodes of epistaxis. His oral acceptance was reduced. Fever was high grade, remittent in nature and a not associated with chills. There was no history of joint pain or swelling, pain abdomen, diarrhea or skin rashes. The child was not receiving any antibiotics. There was history of travelling to a hill station in northern India two months prior to the onset of illness. There was history of consumption of dairy products made from unpasteruized cow milk. There was no history of insect bite or contact with animals or their carcasses. No other family member had similar illness. On examination at admission, child was conscious, well oriented, afebrile with cool extremities, pulse rate was 144/min, low volume, blood pressure was 96/50 mmHg, respiratory rate was 26/min and capillary fill time >3 seconds. There was no pallor, icterus, lymphadenopathy or skin rashes. Throat examination revealed a single whitish exudate over right tonsil with no mucosal congestion. The child had no clinical evidence of arthritis in any joint. He had hepatomegaly of 3.0 cm below costal margin in midclavicular line and splenomegaly of 1.5 cm. There was no abdominal distension or tenderness, no free fluid and bowel sounds were normal. Respiratory and cardiovascular systems were normal clinically. There were no neurological deficit or meningeal signs and fundus examination was also normal. Child had blood counts and widal test done a day prior to admission. Total leucocytic count was 5060 per cu mm with neutrophils 61%, lymphocytes 35%, monocytes 4%, platelet count 1.25 × 105/cu mm, ESR 14 mm 1st hour and no malarial parasite was seen in peripheral smear. Widal test was reported negative (TO <1:80, TH < 1:80, AH < 1:80, BH < 1:80). At admission hemoglobin was 11.2 g/dl, TLC was 3600/cu mm with neutrophils 56%, band forms 9%, platelets 1.30 × 105/cu mm, SGPT (ALT) 254 IU and SGOT (AST) 196 IU. Coagulation profile, CPK, CKMB, renal function tests and serum electrolytes were normal. Dengue serology and monospot test for Epstein Barr virus were negative. Chest radiograph was within normal limits. Gram stain and culture of the throat swab did not show any organism. Patient was started on ceftriaxone and intravenous fluid resuscitation following which peripheral perfusion and BP improved. Blood culture was sterile after 72 hours of incubation by BacTAlert® technique (Organon-Teknika Corporation, Box 15969 Durham, North Carolina, USA).
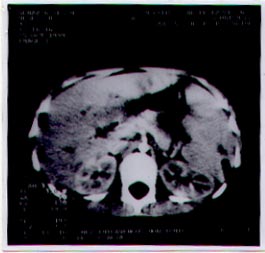
Fig. 1. CT scan abdomen showing hypodense lesion in spleen (arrowed). On day 4 of admission, child developed generalized abdominal pain with severe nausea and nonbilious vomiting. There was generalized abdominal distension with diffuse tenderness. Radiographs of abdomen showed normal bowel gas pattern with no air fluid level or gas under the diaphragam. CT scan abdomen showed hepatosplenomegaly with a single, non enhancing, hypodense lesion in the spleen (Fig. 1) and mild pelvic ascitis. Repeat Hb was 10.5 g/dl and TLC 4000 per cu mm, with neutrophils 81%, myelocytes 3%, metamyelocyte 7%, lymphocytes 8%, eosinophils 1% and platelets 1.2 ´ 105/cu mm. Blood culture was sterile after 72 hours. Mantoux test 5TU-PPD was negative after 48 hours. On day 5 of admission, child was drowsy, sleeping excessively but easily arousable and had headache. Neurological examination including fundus did not reveal any signs of meningitis. CT scan head was normal. Cerebrospinal fluid examination revealed clear fluid containing 6 mononuclear cells with sugar 47 mg/dl and protein 35.4 mg/dl. Gram stain was negative and culture was sterile. Child was also noticed to have developed tender, discreet lymphnodes in submental, submandibular and posterior triangle on both sides of the neck. Size of lymphnodes varied from 1.0 to 1.5 cm. Bilateral axillary lymph nodes, sized 0.5 to 1.0 cm were also noticed. No nodes were palpable in the inguinal region. Tenderness and the size of nodes increased the following day but there was no fluctuation. Bone marrow aspiration showed normocellular marrow with normoblastic erythropoiesis, normal granulocytic series with no maturation abnormality. Increased plasma cells (4%) with unremarkable megakaryocytes and no hemoparasite were reported. Bone marrow culture was later reported sterile. CT scan of thorax showed bilaterial pleural effusion (R>L) with basal atelectasis of lower lobe with no hilar or paratracheal lymphnodes. Viral hepatitis markers, double stranded antinuclear antigen, IgM EBV (viral capsid antigen) and Coomb’s test were negative. Repeat widal test on day 10 of admission (day 15 of illness) did not show rise in titers of any agglutinins. Echocardiography did not show pericardial effusion or vegetation. Agglutination test for Brucella was done on day 10 of admission and was reported positive for B.abortus (1:160). Blood and CSF were sent to Specialty laboratories, Santa Monica, California for Elisa test. IgM for B. abortus were positive only in blood while IgG, IgA in blood and IgM, IgG, and IgA in CSF were negative. During his stay in the hospital, four samples of blood and a bone marrow sample were sent and were incubated for 30 days by BacTAlert® techniques without positive result. Child was treated with oral cotrimoxazole for 6 weeks and intravenous gentamicin for 2 weeks. He became aferbrile within 48 hours and abdominal symptoms and lymphadeno-pathy disappeared within 72 hours of starting therapy and was discharged after 2 weeks of stay in the hospital to complete the treatment at home. Follow up CT scan abdomen done after completion of therapy showed resolution of splenic hypodensity. The child remained afebrile without any evidence of arthritis or arthralgia and hepatosplenomegaly during six months follow-up. Discussion Fever is the commonest clinical manifestation of brucellosis followed by arthralgia, weight loss, poor appetite, malaise and hepatosplenomegaly(4). Arthralgia has been reported in 37-83% of children while arthritis is less common(5). Our patient had fever, dry cough, headache, vomiting with heptosplenomegaly but no arthralgia or arthritis. Unlike in present case who developed tender lymph nodes, only 16% of children are reported to have developed non-tender, discrete lymphadenopathy(4). Hematological findings in brucellosis are reported to be either normal or include anemia, leukopenia, neutropenia, pancytopenia and thrombocytopenia(6). Polymorphonuclear cells more than 75% were reported in only 8% of 400 cases in a series(7). Vallejo et al.(8) reported a child with hepatosplenic abscess with 17% bandemia. No study has reported presence of myelocytes and metamyelocytes in peripheral blood smear. The diagnosis of brucelosis is based on potential exposure, clinical features suggestive of brucellosis and serological tests with or without positive blood culture(9). Serologic tests are the main tools for diagnosis of brucellosis. Serum agglutination test for brucella with titers >1:160 are suggestive of active infection(1). In one report(5) 44% of children from Israel with acute brucellosis had 1:160 brucella agglutinin titers. Elisa test is more sensitive and gives species specific IgM, IgG and IgA and helps in the differentiation of different stages of brucellosis, detects incomplete antibodies and has replaced 2 mercaptoethanol test(11). In the same study all culture positive brucella samples were also positive by Elisa and a significant positive correlation was demonstrated between agglutination test and IgM Elisa. Isolation of brucella organisms from the blood, bone marrow or other tissue fluids is the hallmark of diagnosis. However the rate of isolation from blood is generally low and varies from 15-70%. Use of rapid isolation method (BacTAlert®), prolonged incubation for 30 days and use of bone marrow improve culture positivity(1). In the present case four blood samples and one bone marrow sample were incubated by BacTAlert® technique for 30 days without any yield. Very few case reports are available on CT-scan findings in brucellosis. Valleo et al.(8) reported multiple lesions in the spleen with single liver abscess due to B. melitensis in a young child. Other CT findings reported in a adult patient included dilated small bowel loops with fluid levels and nodular thickening of peritoneum(12). Involvement of lung in brucellosis is rare. Respiratory complications were seen in only 1% of 400 adults(7). Lubani et al.(13) reported 9 cases of pulmonary brucellosis including 5 adults and 4 children out of 400 adults and 1100 children studied in six years period. Massive unilaeral pleural effusion was present in two children in chest radiograph. In the present patient, chest radiographs were normal on two occasions (with a time interval of more than a week). In a study of 165 cases, 83.6% had normal chest radiograph(14). CT scan thorax in our patient revealed bilaterial pleural effusion with basal atelectasis. This finding has not been reported in pediatric and adult studies on brucellosis in English literature. Our case received ceftriaxone for first seven days but fever did not respond. A similar observation has been reported in earlier literature(15). The present patient of acute brucellosis had certain unusual features which include appearance of tender lymphadenopathy in both cervical and axillary regions, neutrophilic predominance with shift to left, bilaterial pleural effusion and solitary splenic hypo-density with pelvic ascitis in CT scans of thorax and abdomen, respectively. Though blood and bone marrow cultures did not grow brucella organisms, positve aglutination test and brucella IgM by Elisa test in a child with history of exposure led to the diagnosis of Brucella abortus infection which is known to cause benign disease as compared to B. melitensis. Contributors: AS conceived and drafted the case report and will act as a guarantor for the paper. SB contributed to case study and literature search. RV was resposible for the radiological workup. Funding: None. Competing interests: None stated.
| ||
| References | ||
|
![]()