|
Case Reports Indian Pediatrics 1999;36:1267-1270 |
Cornelia de Lange Syndrome: Discordance in Twins |
| Sheela S.R. From the Department of Pediatrics, Samaritan Hospital,
Kizhakkambalam P.O., Alwaye 683 562, Ernakulam District, Kerala, India. |
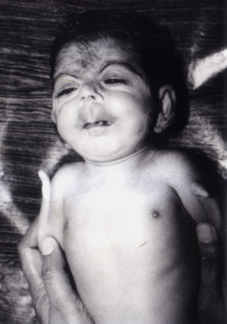
| It is extremely rare for Cornelia de Lange syndrome to occur in one of a pair of twins; only one such case has been reported so far(1). I am reporting this case because of its rarity. Case Report A 32-year-old mother, underwent Caesa-rean section for twin pregnancy with transverse lie. The first born of twins was a female baby weighing 1500 g with a gestational age of 34 weeks. Apgar score was 6 and 9 at 1 and 5 minutes, respectively. The other twin was a perfectly normal male baby weighing 2.75 kg. The elder sibling is a normal female child who is 5 years old. There is no family history of consanguinity. Physical examination of the first twin revealed a 34 week preterm SGA baby weighing 1500 g, with a length of 38 cm and a head circumference of 27 cm. Baby was hirsute, with excess hair over the forehead and ears and upper back, with a low posterior hair line; she had bushy eyebrows and synophrys, and long curly eyelashes. The face showed anteverted nostrils and a long philtrum; the lips were thin with a small midline beak of the upper lip and a corresponding notch in the lower lip, with a downward curving of the angle of the mouth (Fig. 1).
Fig. 1. Photograph showing characteristic lips and mouth, long philtrum, bushy eye brows, hirsutism and anteverted nostrils. The baby had severe micrognathia with glossoptosis, high arched palate and midline cleft of the soft palate, and a low pitched cry. The nipples were hypoplastic. Skeletal abnormalities included phocomelia with oligodactyly (single finger) in both upper limbs, flexion contracture of elbows and syndactyly of the second and third toes (Fig. 2).
Fig. 2. Photograph showing phocomelia and oligodactyly of both upper limbs. X-ray of both upper limbs showed presence of single bone in both fore-arms with single finger in each hand (Fig. 3). The baby also had a sub-aortic VSD, confirmed by color Doppler Echo. Baby expired following an aspiration bronchopneumonia when she was four months old.
Fig. 3. X-ray chest with both upper limbs showing single forearm bone and single finger in each hand. Discussion Cornelia de Lange syndrome (Brachmann_de Lange syndrome) was originally reported in 1933 by Cornelia de Lange. Brachmann had described a child with similar feature at autopsy in 1916. These patients manifest both prenatal and postnatal growth retardation. They are mentally retarded, IQ varies from below 30 to 86 with an average of 53; those with higher IQs tend to have better weight and head circumference(2). A characteristic feature of this syndrome is bushy eyebrows with synophrys, and long curly eyelashes, associated with hirsutism. Other common features include microbrachycephaly with initial hypertonicity and a low pitched weak cry. The typical facial features include a depressed nasal bridge with anteverted nostrils, a long philtrum, a thin upper lip and downturned angles of the mouth. The palate is usually high arched. Late eruption of widely spaced teeth and micrognathia are common. Limb anomalies are usual and include micromelia (93%), phocomelia and oligodactyly (27%), flexion contracture of the elbows (64%), syndactyly of the second and third toes (64%) and clinodactyly of fifth fingers(2). Males may have hypoplastic genitalia, undescended testes and hypospadias. Ocular anomalies include myopia, ptosis and nystagmus. Study of the auditory brain stem evoked responses have shown high prevalence of sensorineural hearing deficit(3). Autistic or self destructive behavior may be noted. Congenital heart disease, usually VSD, is an occasional finding. These patients have feeding problems related to swallowing incoordination, poor esophageal motility, and gastro-esophageal reflux. Gastro intestinal anomalies including malrotation, colonic duplication and non-fixation of the colon are also described(4). Death is usually due to complications following aspiration(2). Structural defects occur two to three times more commonly in live born monzygotic twins (MZ) than in dizygotic twins. Among MZ twins, malformations are most common in the monochorionic_monoamniotic twins. The defects that occur with increased frequency in MZ twins are sacrococcygeal teratoma, sirenomelia, VATER association, anencephaly and holoprocencephaly(2). About 5-20% of such cases are concordant. The incidence of concordance in a dizygotic twin is of similar magnitude to that of siblings born of separate pregnancies, suggesting that environmental factors are unlikely to be of major importance. The unusual feature in this case is a female twin with typical features of Cornelia de Lange syndrome while the other male twin is a perfectly normal baby. This has been mentioned in the literature only in a single similar case(1). This female baby with Cornelia de Lange syndrome had phocomelia and oligodactyly involving both upper limbs, which is seen only in 27% of patients with this syndrome(2,5). A study conducted among 64 individuals with this syndrome showed that lower birth weight correlates with a more severe phenotype specifically including severe upper limb malformation and greater psychomotor retardation; the lower birth weight group showed a significant excess of females(6). The case mentioned here correlates well with their observation. A survey of speech and language skills was conducted in 116 patients with this syndrome to ascertain the prognostic value of related variables. Children who were not talking at all or who were severely delayed in language skills had at least one of the following characteristics: birth weight under 5 lbs, a reported diagnosis of moderate to severe hearing impairment, upper limb malformations, poor ability to relate socially and severe motor delays(7). The case described here had two variables, i.e., a birth weight below 5 lbs and upper limb malforma-tion, showing a high probability for a serious speech defect had she survived. The etiology of this syndrome is unknown. Most cases are sporadic. The recurrence risk in 377 siblings of 310 patients with Cornelia de Lange syndrome was calcualted to be less than 1%(5). Autosomal dominant inheritance has been suggested based on four instances in which a mildly affected parent and one or more of his/her children were affected(8). Chromosomal analysis of patients with this syndrome revealed duplication of the q 26-27 band region of chromosome 3(2,9). Low levels of pregnancy associated plasma protein A (PAPPA) has been suggested as a biochemical indicator of pregnancies with aneuploid fetuses. Complete absence of PAPPA in pregnancies associated with Cornelia de Lange syndrome has suggested a causal connection between PAPPA and the development of this syndrome thus making PAPPA a possible marker in the prenatal diagnosis of Cornelia-de Lange syndrome(10). References 1. Stevenson RE, Scott CI Jr. Discordance for Cornelia de Lange syndrome in twins. J Med Genet 1976; 13(5): 402-404. 2. Jones KL. Smith's Recognizable Patterns of Human Malformation, 5th edn. Philadelphia, W.B. Saunders Co, 1997; pp 88-91. 3. Kaga K, Tamai F, Kitazumi E. Auditory brain stem responses in children with Cornelia de Lange syndrome. Int J Pediatr Otorhinolaryngol 1995; 31: 137-146. 4. Husain K, Fitzgerald P, Lau G. Caecal volvulus in the Cornelia de Lange syndrome. J Pediatr Surg 1994; 29: 1245-1247. 5. Jackson L, Kline AD, Barr MA, Koch S. De Lange syndrome: A clinical review of 310 individuals. Am J Med Genet 1993; 47: 940-946. 6. Hawley PP, Jackson LG, Kurnit DM. Sixty four patients with Brachmann-de Lange syndrome: A survey. Am J Med Genet 1985; 20: 453-459. 7. Goodban MT. Survey of speech and language skills with prognostic indicators in 116 patients with Cornelia-de Lange syndrome. Am J Med Genet 1993; 47: 1059-1063. 8. Robinson LK, Wolfsberg E, Jones KL. Brachmann-de Lange syndrome: Evidence for autosomal dominant inheritance. Am J Med Genet 1985; 22: 109. 9. Wilson GN, Heiber VC, Schmickel RD. The association of chromosome 3 duplication and the Cornelia de Lange syndrome. J Pediatr 1978; 93: 783-788. 10. Silahtaroglu AN, Tumer Z, Kristensen T, Sottrup_Jensen L, Tommerup N. Assignment of the human gene for pregnancy associated plasma protein A (PAPPA) to 9q 33.1 by fluorescence in situ hybridization to mitotic and meiotic chromosomes. Cytogenetics Cell Genet 1993; 62: 214-216. |