|
|
|
Indian Pediatr 2016;53: 747-748 |
 |
En-masse Protrusion of Ventriculo-peritoneal
Shunt Tube Through the Anus
|
|
*T Renu Kumar and #M Sai Sunil Kishore
*Department of Pediatric Surgery and #Pediatrics,
Maharaja Institute of Medical Sciences, Nellimarla, Vizianagaram Andhra
Pradesh, India
Email: [email protected]
|
|
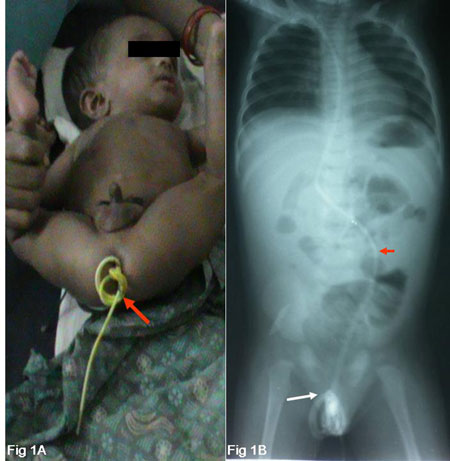
A 7-month-old boy, with a right-sided Ventriculo-peritoneal (VP) shunt
in-situ for 2 months, presented with shunt tube protruding
through anus for 2 hours. The infant was treated for acute diarrhea till
2 days ago. There were no signs of meningitis or peritonitis. Perineum
showed a ‘bunch of shunt coils’ dripping cerebrospinal fluid (Fig.
1). Abdominal X-ray showed point of entry of the shunt
tube into the sigmoid colon with no pneumoperitoneum (Fig 1).
The shunt was divided through small subcostal incision; cranial end was
removed and the peritoneal end was pulled out through anal opening.
 |
|
Fig. 1 (a) Infant with ‘bunch of
coils’ of shunt tube protruding through the anus with securing
sutures in situ (red arrow); (b) Abdominal X-ray showing point
of shunt entry into the sigmoid colon (red arrow) and shunt
coils lying in the perianal region(white arrow).
|
Besides infection, malfunction, and CSF loculations,
the shunt tube can migrate into any visceral organ [1]. Intestinal
perforation caused by shunt procedures is rare, and about 50% occur in
infants. Anal protrusion of shunt is an extremely rare complication
[1,2].
Often, some surgeons keep sufficient length of shunt
tube to accommodate for the linear growth of the baby by coiling the
peritoneal end and securing the ‘bunch of coils’ with an absorbable
suture in the supra-hepatic space so that shunt does not spread itself
all over the peritoneal cavity between the intestinal loops. This
decreases the chances of intestinal perforations and spontaneous
knotting. Despite this effective technical modification to tackle
peritoneal complications, anal protrusion still occurred in this child,
and the entire ‘bunch of intact coils’ of shunt protruded en-masse
through the anus without any peritonitis. Such protrusion should create
a big rent in the eroded sigmoid colon or cause peritonitis but
strangely there was none, suggesting that shunt erosion is a slow
process where erosion and healing by shunt induced adhesions takes place
simultaneously to conceal a free perforation. The shunt tip adheres and
erodes the bowel by continuous friction, and is then propelled distally
by peristalsis to protrude anally [3,4]; diarrhea may further aggravate
the process of protrusion.
Mechanisms responsible for silent erosion and anal
protrusion are multifactorial. Predisposing factors for anal protrusions
are stiff shunt tube, thin bowel wall with strong peristalsis in
infants, malnutrition, infection and foreign body reaction. Exaggerated
peristalsis in diarrhea can predispose to en-masse protrusion of
shunt coils. Redundant sigmoid colon is the most favorable site for
shunt erosion and subsequent anal protrusion. Abdominal X-ray
does not show pneumoperitoneum because shunt perforations are usually
concealed. Anal protrusion of shunt without peritonitis is treated by
percutaneous division and removal of the cranial end, and the peritoneal
end is pulled out through the anus [3,5]. The perforation is usually
sealed by a chronic fibrous sheath around the shunt track, and
laparotomy is usually not required [3,5].
References
1. Ho KJ. Recurrent meningitis associated with
intragastric migration of a ventriculoperitoneal shunt catheter in a
patient with normal-pressure hydrocephalus. South Med J. 1992;85:1145-8.
2. Sathyanarayana S, Wylen EL, Baskaya MK, Nanda A.
Spontaneous Bowel Perforation after ventriculoperitoneal shunt surgery:
Case report and a review of 45 cases. Surg Neurol.
2000;54:388-96.
3. Digray NC, Thappa DR, Arora M, Mengi Y, Goswamy
HL. Silent bowel perforation and transanal prolapse of a
ventriculoperitoneal shunt. Pediatr Surg Int.
2000;16:1;94-5.
4. Ansari S, Nejat F, Dadmehr M. Extrusion of
ventriculoperitoneal shunt catheter through the rectum and retrograde
meningitis. Pediatr Infect Dis J. 2005;24:1027.
5. Jamjoom AB, Rawlinson JN, Kirkpatrick JN. Passage
of tube per rectum: An unusual complication of a ventriculoperitoneal
shunt. Br J Clin Pract. 1990;44: 525-6.
|
|
|
 |
|
