|
|
|
Indian Pediatr 2016;53:
727-729 |
 |
Reversible Cerebral
Atrophy in Infantile Tremor Syndrome
|
|
Rajesh Gupta, Ashish Pathak, Jagdish Mandliya,
*Prateek Gehlot and
#Pavan Sonker
From Department of Pediatrics. *Radiology and #Biochemistry,
RD Gardi Medical College, Ujjain, MP, India.
Correspondence to: Dr Rajesh Gupta, B-6/5, Doctor’s
quarters, RD Gardi Medical College, Surasa, Ujjain, MP, India.
Email: [email protected]
Received: September 10, 2015;
Initial review: October 20, 2015;
Accepted; March 10, 2016.
Published online: June 01, 2016. PII:S097475591600002
|
Background: We report changes in MRI brain of children with
Infantile Tremor Syndrome (ITS) at the onset of illness and following
treatment. Case characteristics: Three children with infantile
tremor syndrome were assessed for changes in brain neuroimaging at
admission and at follow-up visit. On MRI, all children had mild to
severe diffuse cerebral atrophy, which reverted back to normal on
follow-up visits. Outcome: Children with infantile tremor
syndrome have reversible diffuse cerebral atrophy on neuroimaging.
Key words: Management, Outcome, Tremors.
|
|
I
nfantile Tremor Syndrome (ITS) is a clinical
state characterized by tremors, anemia, pigmentary skin disease,
regression of mental development, and hypotonia of muscles [1]. Studies
suggest that the most probable etiology of ITS is nutritional
deficiencies [1]. Despite predominance of neurological symptoms, very
few studies have documented neuroanatomical and/or neurophysiologic
changes in ITS [2]. Reduced brain substance has been documented in
children with ITS [3]. In contrast several studies in children with
Protein Energy Malnutrition (PEM) have documented cerebral atrophy [4,5]
and its reversibility after treatment [5].
We report three cases of ITS diagnosed clinically
based on above definition with MRI findings described at diagnosis and
on follow-up after 6-18 months. All patients were treated with WHO
protocol for management of undernutrition with or without propranolol to
control tremors. Developmental Quotient (DQ) of all cases was assessed
using Developmental Screening Test (DST). Written informed consent was
obtained from parents of all the children.
Case Report
Case 1
A 10-month-old exclusively breastfed female child was
admitted with the complaints of abnormal rhythmic jerky movements of
both hands, feet, tongue and head nodding for 6 days prior to admission.
Movements were suggestive of coarse resting tremors. Child was having
moderate wasting and normal height for age. Head circumference was below
–2 SD for age and sex. Developmentally, child was able to sit without
support, had a palmar grip, and was able to tell monosyllables before
the onset of disease (DQ 92±5). At admission, she was not able to sit
without support and only cooing was present (DQ 44±5). Blood
investigations suggested predominantly microcytic hypochromic anemia
with normal serum levels of albumin and Vitamin B 12.
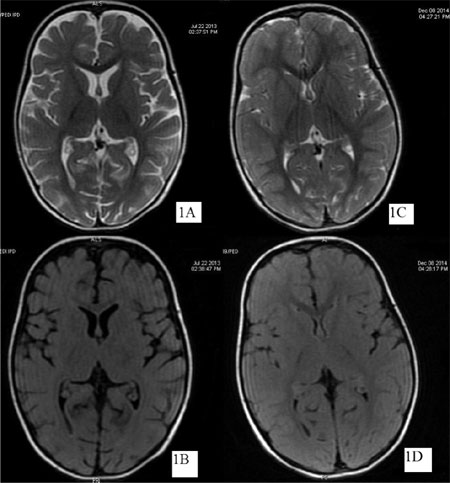
MRI brain suggested mild diffuse cerebral atrophy (Fig.1a
and 1b). Nutritional rehabilitation was continued at home after 5
days of admission. Follow-up of the patient was done after 17 months
when she had normal development for her age (DQ 84±5).
Anthropometrically she had normal weight for age, and length. Head
circumference was still below -2 SD. MRI scan of brain showed
improvement in cerebral atrophy with no sulcal prominence or ventricular
enlargement (Fig.1c and 1d).
Case 2
An 8-month-old exclusively breastfed female child
admitted with abnormal rhythmic movements of tongue and upper
extremities and tremulous cry, along with loose motions for two days.
She was having normal weight for height and mild stunting with head
circumference <-2SD. She had normal development before illness (DQ 90±5)
with regression of milestones during tremors (DQ 74±5). Child was mostly
remaining in a flexed posture with fisting of the palms. Tremors used to
increase on crying but disappeared on sleep. She stayed in hospital for
11 days and was treated with oral rehydration solution, Zinc sulfate,
Vitamin B12 and Folic acid.
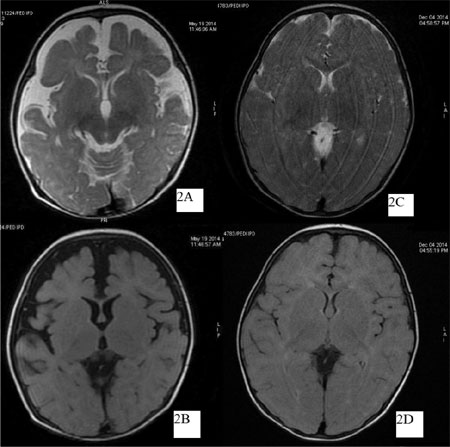
Propranolol was given to control tremors. Blood investigations suggested
normocytic hypochromic anemia with normal serum levels of albumin and
Vitamin B12. MRI brain was
suggestive of mild diffuse cerebral atrophy (Fig. 2a and
2b), which showed reversal of atrophy on follow up after 15
months (Fig. 2 c and 2d) with normal development
(DQ 100±5).
Case 3
A 13-month-old female with inadequate complementary
feeding was admitted with complaints of not able to sit for about 6
weeks, cough for 4 days and abnormal cry, head nodding and rhythmic
movements in extremities for one day. Severe pallor was present along
with knuckle hyper-pigmentation. Child was having severe wasting, mild
stunting and head circumference <-1SD (DQ 25±5). Blood investigations
showed moderate polychromasia, mild anisopoikilocytosis, mainly
normocytes, tear drop cells, target cells with normal serum albumin and
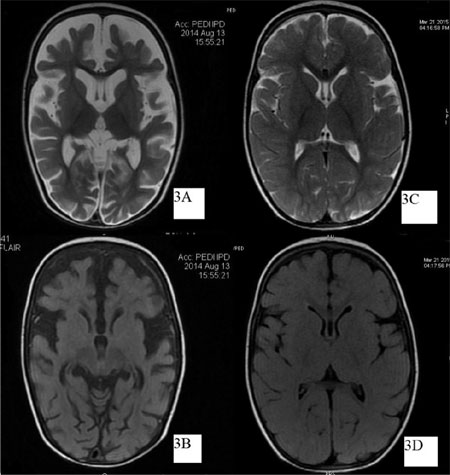
sub-normal serum vitamin B 12
levels. MRI brain suggested diffuse cerebral atrophy with prominent CSF
spaces including sulci and sylvian fissures of both hemispheres and
enlarged lateral ventricles (Fig. 3a and 3b).On
follow-up, child was again admitted at the age of 20 months.
Anthropometrically she had normal weight for height with mild stunting
and mid arm circumference 14 cm. Head circumference was <-1SD with
normal development (DQ 78±5). MRI brain showed reversal of atrophy and
it revealed minimal residual prominence of sylvian fissures (Fig.
3c and 3d).
Discussion
We demonstrated reversibility of cerebral atrophy by
MRI brain in cases of ITS, after nutritional rehabilitation. All three
cases had various grades of cerebral atrophy on MRI during acute tremor
phase of ITS. Bajpai, et.al. [3] observed a reduced brain
substance with normal sized skull in majority of cases of ITS on
Pneumoencephalo-graphy [3]. Other cross-sectional studies [2,6] have
done CT/ MRI scan during tremor phase of ITS and demonstrated cerebral
atrophy, but none of these studies did follow-up neuroimaging. Ozer EA,
et al. [7] described two cases of tremors in infantile
cobalamin deficiency and cerebral atrophy on CT scan [7]. However,
cobalamin deficiency is not constantly present in all patients of ITS,
as shown in our series in which only one child had sub-normal vitamin B 12
levels.
Reversibility in cerebral atrophy has not been
documented in reference to ITS. Previous studies have reported
reversible cerebral shrinkage in Kwashiorkor on MRI of twelve children
aged 6 to 37 months [5]. At 90 days, the cerebral changes had resolved
in nine and improved substantially in the remainder. Improvement in
brain size was apparent on day 30 of nutritional rehabilitation in the
majority of Kwashiorkor patients. This improvement in brain size was
attributed to fluid shifts between various compartments and to a lesser
degree to fat or protein abnormalities in the brain. It is postulated
that fluid moves out of intravascular spaces as a result of decreased
colloid osmotic pressure, floods the subarachnoid spaces, dilates the
ventricles, and widens the cisternal spaces and sulci. When nutrition is
improved the plasma proteins rise, the extracellular fluid moves back
into the intravascular space [5]. In our case series, no patient had
reduced levels of serum albumin on admission, therefore the above theory
does not explain the reversible cerebral atrophy in our patients.
A 11-month-old infant with malnutrition, failure to
thrive and marked cortical atrophy on brain CT has previously been
described [8]. Improvement of the maternal-infant relationship, combined
with appropriate nutrition, transformed the infant within 2 months into
a normally developing baby with body weight and head circumference
within the normal percentile range. A corresponding improvement was
found in the brain CT [8].
All our cases on follow-up showed marked improvement
in their anthropometric and developmental measures. The corresponding
neuroimaging reversibility of cerebral atrophy suggests the role of
dietary management along with social stimulation and support. Primarily
ITS seems to be related to undernutrition [1] and is reversible with
nutritional rehabilitation. Therefore, this series suggests a neuro-anatomical
evidence of effectiveness of nutritional rehabilitation in management of
ITS.
Contributors: RG, AP, JM: involved in the study
concept, designing and manuscript writing; RG: did assessment of
patients; PG: did radiological assessment; PV: did biochemical analysis.
The final manuscript was approved by all authors.
Funding: None; Competing interest: None
stated.
References
1. Gupta BD, Maheshwari RK, Miglani N. Infantile
tremor syndrome. Indian J Pediatr. 1978;45:221-8.
2. Thora S, Mehta N. Cranial neuroimaging in
Infantile tremor syndrome. Indian Pediatr. 2007;44:218-9.
3. Bajpai PC, Mishra PK, Tandon PN. Further
observations on infantile tremor syndrome. Indian Pediatr.
1968;5:297-307.
4. Tatawy S, Badrawi N, El Bishlawy A.
Cerebral atrophy in infants with protein energy malnutrition. Am J
Neuroradiol. 1983;4:434-6.
5. Gunston GD, Burkimsher D, Malan H, Sive AA.
Reversible cerebral shrinkage in kwashiorkor: An MRI study. Arch Dis
Childhood. 1992;67:1030-2.
6. Goraya JS, Kaur S. Infantile tremor syndrome –
down but not out. Indian Pediatr. 2015;52:250.
7. Ozer EA, Turker M, Bakiler AR, Yaprak I, Ozturk C.
Involuntary movements in infantile cobalamin deficiency appearing after
treatment. Pediatr Neurol. 2001;25:81-3.
8. Kessel A, Tal Y, Jaffe M, Even L. Reversible brain
atrophy and reversible developmental retardation in a malnourished
infant. Isr J Med Sci. 1996;32:306-8.
9. Mishra PK, Tandon PN, Bajpai PC. Infantile tremor syndrome –
probable etiology. Indian Pediatr. 1971; 8:63-4.
|
|
|
 |
|