|
|
Research Papers Indian Pediatrics 2008; 45: 661-667 |
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
Single versus Multiple Courses of Antenatal Betamethasone and Neonatal Outcome: A Randomized Controlled Trial |
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
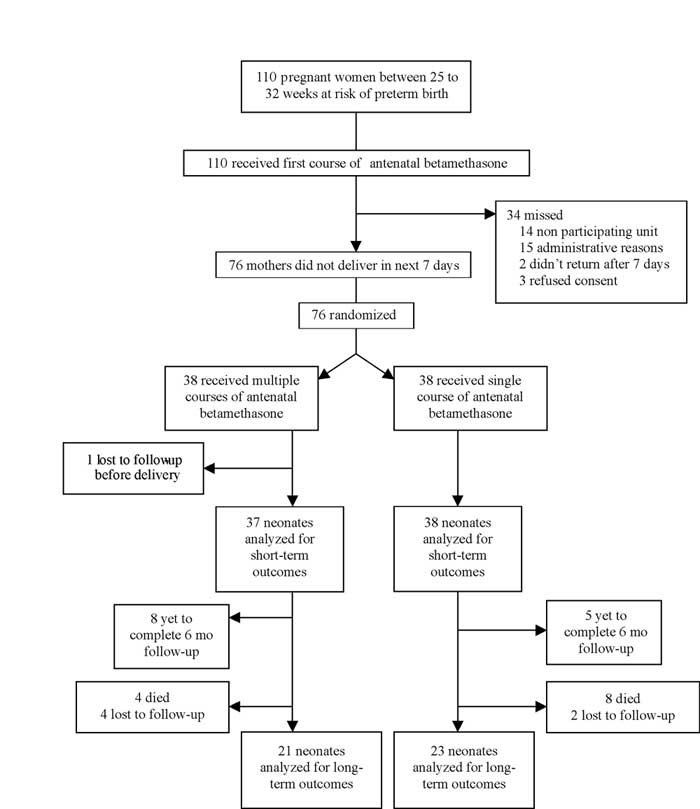
Introduction The use of antenatal corticosteroids has significantly reduced the incidence of respiratory distress syndrome (RDS), intraventricular hemorrhage (IVH), necrotizing enterocolitis (NEC), sepsis and overall neonatal mortality(1). In 1994, National Institutes of Health (NIH) recommended the administration of a single course of antenatal corticosteroids for women at risk of preterm birth presenting between 24-34 weeks of gestation(2). It is believed that the course of antenatal steroids is maximally beneficial if the newborn is delivered after 24 hours and within 7 days of the last dose of steroid. Weekly courses of antenatal steroids have been proposed on this basis. The major concern of those opposing multiple courses has been the adverse outcomes on growth and neuro-development(3). Many others opine that neonatal morbidity and mortality decreases after repeated courses of antenatal steroids with no significant adverse effects(4-5). The NIH has recommended that, multiple courses should be used only in the context of well-conducted randomized controlled trials (RCT)(6). There is a paucity of data on this issue from developing countries. In the context of inaccessibility and unaffordability of advanced neonatal interventions, a low cost universally accessible intervention such as multiple courses of antenatal corticosteroids has immense potential. We hypothesized that multiple courses of antenatal betamethasone would reduce short-term neonatal morbidity without adversely affecting growth and neurodevelopment at 6 months, when compared to a single course. Methods This study was an open-labeled, RCT conducted in a tertiary care hospital of northern India from August 2004 onwards. Data from a previous cohort study in this unit had showed that 6% babies in the multiple courses antenatal corticosteroid group and 33% in the single course antenatal corticosteroid group had severe RDS(7). To detect this difference with a 2-tailed alpha of 5% and beta of 20%, 70 subjects were required. Participants: Mothers who presented from 25 to 32 completed weeks of gestation with a risk of preterm delivery were given a standard course of antenatal betamethasone (12 mg intramuscularly, 2 doses 24 hours apart) as per the unit policy. They were administered tocolytics and antibiotics depending on the clinical indication. For the purpose of this study, these pregnant women were tracked daily. If they did not deliver by 7 days of the first dose of the antenatal betamethasone course, they were included, provided they were available for follow-up every week until delivery. Mothers with unreliable gestation, frank clinical chorioamnionitis or major fetal congenital malformations were excluded. In case of multiple gestations, only the first-born neonate was evaluated for outcomes. This is because second and higher order born babies have a significantly higher risk of RDS. Written informed consent was obtained from all participants. The study was approved by the Institute Ethics Committee. Intervention: Baseline information regarding demographic and obstetric data was recorded in a structured proforma after enrolment. Subjects were randomized to receive single or multiple courses of betamethasone intramuscularly (12 mg 24 hourly for 2 doses) until delivery or 34 weeks of gestation, whichever was earlier; by a process of simple randomization, using a website-generated random number list. Slips bearing the random allocation were placed in opaque envelopes, sealed and numbered serially on the outside. All newborns were assessed for development of respiratory distress syndrome (RDS), intra-ventricular hemorrhage (IVH), necrotizing enterocolitis (NEC), patent ductus arteriosus (PDA), bronchopulmonary dysplasia (BPD), sepsis and retinopathy of prematurity (ROP). Their occipito-frontal circumference (OFC), weight, and length at birth were measured. The OFC, weight and length, and neurodevelopment were again evaluated at 6 months corrected age. Assessments of neonatal outcomes and interim follow-up have been completed, but the final follow-up at 18 months is awaited. Outcome measures: The primary outcome was incidence of severe respiratory distress syndrome. RDS was defined as onset of respiratory distress within 6 hrs of birth in a preterm with either negative gastric shake test or a chest x-ray showing poor expansion, air bronchogram or reticulogranular pattern. Severe RDS was defined as RDS requiring mechanical ventilation for at least 12 hours. Indications for mechanical ventilation were: if on CPAP (maximum 8 cm, FiO2 0.8), the patient had hypoxemia (PaO2 <50 mm Hg) or hypercapnic acidosis (PaCO2 >50 mm Hg with pH <7.25) or worsening acidosis (either respiratory or metabolic) or clinically evident worsening respiratory fatigue/apneas or work of breathing. CPAP alone was not included in "mechanical ventilation" because of the unit policy of giving "early CPAP". Secondary outcomes were incidence of non-severe RDS, IVH, NEC, PDA, BPD, sepsis, ROP and deaths within 28 days; birthweight, length and OFC; development and growth parameters at 6 months corrected age. IVH, NEC, PDA, BPD, sepsis and ROP were diagnosed based on standard criteria(8). "Deaths within 28 days" included stillbirths and neonatal deaths. Birth weights were measured using an electronic weighing balance with a least count of 5 grams (Indosaw, Oswal industrial products, Ambala).Weights during follow-up were taken using a weighing balance with a least count of 100 g (Avery Berkel, West Midlands, England). OFC was measured using a non-stretchable tape placed firmly around the head with the following reference points: supraorbital ridge anteriorly and the most prominent point of occiput posteriorly. Length was measured using an infantometer. Amiel Tison’s method of neurological examination was used(9) and neuro-logical examination was considered abnormal in the presence of tone abnormalities, disturbed cortical function or persistent primitive reflexes. Develop-ment was evaluated by Denver Development Screening Test II(10). Standard unit policies, including those of giving surfactant and ventilation were followed in all enrolled subjects. Statistical analysis: Baseline variables were described by descriptive statistics. Normally distributed numerical variables were compared by Student’s t test; skewed distributions were compared by Mann Whitney U test, and dichotomous variables were compared by Chi square test with continuity correction or Fisher’s exact test, as applicable. Results Figure 1 depicts the enrollment and randomization of pregnant women. The average number of courses of antenatal betamethasone received by multiple course group was 2.94. In the multiple course group, 3, 15, 7, 8, 3 and 2 mothers received 1, 2, 3, 4, 5 or 6 doses of steroids, respectively, Eighty-three babies were born to 75 mothers, including 6 pairs of twins and one triplet. There was one stillbirth in single course group. Thus, there were 37 neonates each in the 2 groups, for evaluation of primary outcome and short-term morbidity. For comparison of outcomes that included death, the stillbirth in single course group was also included. Baseline variables were similar on comparing the two groups (Table I).
TABLE I Comparison of Baseline Characteristics in the Two Groups
*Denominator N=37 as one mother left before delivery Table II compares the neonatal morbidity, mortality and anthropometry in the two treatment arms. There was no significant difference in the incidence of severe RDS between the two groups. Among severe RDS, one baby received surfactant for early rescue therapy. This baby was in single course group and needed ventilation for 17 hours. Among non-severe RDS, one baby who received surfactant for early rescue therapy by the INSURE technique, belonging to single course group. Two babies needed early CPAP in multiple course and 3 in single course group. All morbidity, mortality and birth anthropometry were similar in the 2 groups. Only the composite outcome of "any RDS and/or death within 28 days" had a trend to be less in multiple course group. TABLE II Comparison of Neonatal Outcomes Between the Two Groups
*Where death was not part of outcome, N= 37 was denominator (i.e. excluding stillbirth). Figure in brackets are percentages. RDS= respiratory distress syndrome, OFC= occipito-frontal circumference. Other outcomes that could potentially alter the incidence of RDS, such as gestational age at delivery, mode of delivery, fetal distress and birth asphyxia were also compared and no significant differences were found (P>0.05). Table III compares the postnatal growth and neuro-developmental outcome by 6 months in the 2 groups. The length and weight, but not OFC, were significantly lower in the multiple course group. A significantly greater proportion of infants in the multiple course group had length, weight and OFC less than 25th centile. At 6 months, 5 babies in the multiple course group were on exclusive breast feeding, 5 on mixed feeding, 6 were receiving non-human milk and 5 babies had been started on weaning foods along with cow’s milk. In the single course group, 6 were on exclusive breastfeeding, 7 on mixed feeding, 3 were receiving non-human milk and 7 babies had been started on weaning foods along with cow’s milk. These differences were not significant. TABLE III Comparison of Post-natal Outcomes at 6 Months Corrected Age
Figures in brackets are percentages: OFC= occipito-frontal circumference. Discussion This study showed that there was no significant benefit of multiple courses of antenatal beta-methasone over a single course in threatened preterm deliveries with respect to severe RDS or for any of the other neonatal morbidities. This study was not adequately powered for secondary outcome measures. Weight and length were significantly lower at a corrected age of six months in subjects exposed to multiple courses of antenatal betamethasone. Our results are similar to some of the older studies(11,12), but are contrary to the results of the more recently conducted, well-designed RCTs(13-15), which reported a significant decrease in RDS, severe lung disease and need for surfactant in babies exposed to the multiple antenatal betamethasone courses. Our study had a smaller sample size compared to the recent large RCTs, which may explain why a significant difference could not be detected. Our unit policy is to give early rescue natural surfactant (less than 2 hrs) in preterm infants of gestation less than 34 weeks with a clinical presentation of RDS, only if the parents can afford to buy surfactant. Surfactant is also given to babies on CPAP, and mechanical ventilation is not a pre-requisite. Conclusions drawn from our study can only be extrapolated to settings similar to ours. The major fear with corticosteroid use is the long term effects of corticosteroids on growth and neurodevelopment. This study showed a significant lowering of weight and length and their corresponding velocities at a corrected age of 6 months. The growth faltering at six months in this study might be indicative of further growth failure at later ages. Such concerns have been voiced by other authors as harbringer of later neurodevelopmental morbidity(16,17). There was no significant difference in the neuro-developmental outcome evaluated at corrected age of six months between the two groups in our study. This study was not adequately powered to pick up a difference at 6 months. Ideally, an evaluation at 18 months corrected age is a more appropriate time to evaluate neurodevelopment(16,18,19). We plan to continue follow-up until 18 months corrected age and make renewed efforts to contact those who did not follow-up at 6 months corrected age. Contributors: PM recruited subjects, collected data and wrote the manuscript. SD designed the study, analyzed data and edited the manuscript, JK helped in recruitment of mothers, AN supervised planning the study, analysis of data and editing the manuscript. Funding: None. Competing interests: None stated.
| ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
![]()